General Information About Late Effects of Treatment for Childhood Cancer
During the past five decades, dramatic progress has been made in the development of curative therapies for pediatric malignancies. More than 80% of children with cancer who have access to contemporary therapies are expected to survive into adulthood.[1] The therapies responsible for this survival can also produce adverse, long-term, health-related outcomes, referred to as late effects, which appear months to years after completion of cancer treatment.
Many approaches have been used to study the very long-term morbidity associated with childhood cancer and its contribution to early mortality. These initiatives have used a spectrum of resources, including data from the following:
- Population-based registries.[2,3]
- Self-reported outcomes (provided through large-scale cohort studies).[4,5]
- Medical assessments.[6,7,8]
High-quality data is needed to establish the occurrence of and risk profiles for late cancer treatment–related toxicity. The highest quality data typically comes from studies that report outcomes in survivors who have undergone medical assessments that provide well-characterized clinical statuses, treatment exposures, and specific late effects. Regardless of study methodology, it is important to consider selection and participation bias of the cohort studies in the context of the findings.
Prevalence of Late Effects in Childhood Cancer Survivors
Late effects are common in adults who have survived childhood cancer. Their prevalence increases as time from cancer diagnosis elapses. Multi-institutional and population-based studies have shown excess risk of hospital-related morbidity among childhood and young adult cancer survivors compared with age- and sex-matched controls, with some evidence that this risk is disproportionately high among survivors of racial and ethnic minority populations.[3,9,10,11,12,13]
Among adults who were treated for cancer during childhood, late effects contribute to a high burden of morbidity. Research has shown the following:[4,7,14,15,16,17,18]
- 60% to more than 90% of survivors develop one or more chronic health conditions.
- 20% to 80% of survivors experience severe or life-threatening complications during adulthood.
- Morbidity accumulation is accelerated in young adult survivors of childhood cancer, compared with that of siblings and the general population. Accumulation of chronic diseases predicts risk of early mortality.[19]
The St. Jude Life (SJLIFE) cohort study aimed to describe the cumulative burden of cancer therapy using the cumulative burden metric, which incorporates multiple health conditions and recurrent events into a single metric that takes into account competing risks. By age 50 years, survivors in this cohort experienced an average of 17.1 chronic health conditions, 4.7 of which were severe/disabling, life threatening, or fatal.[16] This finding contrasts with the cumulative burden in matched community controls, who experienced 9.2 chronic health conditions, 2.3 of which were severe/disabling, life threatening, or fatal (see Figure 1).[16]

Figure 1. Figure shows distribution of cumulative burden by age among childhood cancer survivors of specific pediatric cancer subtypes and community controls participating in the SJLIFE cohort study. The cumulative burden at age 30 years and rate of cumulative burden growth is variable across cancer subtypes and organ systems. Reprinted from The Lancet, Volume 390, Issue 10112, Bhakta N, Liu Q, Ness KK, Baassiri M, Eissa H, Yeo F, Chemaitilly W, Ehrhardt MJ, Bass J, Bishop MW, Shelton K, Lu L, Huang S, Li Z, Caron E, Lanctot J, Howell C, Folse T, Joshi V, Green DM, Mulrooney DA, Armstrong GT, Krull KR, Brinkman TM, Khan RB, Srivastava DK, Hudson MM, Yasui Y, Robison LL, The cumulative burden of surviving childhood cancer: an initial report from the St Jude Lifetime Cohort Study (SJLIFE), Pages 2569–2582, Copyright (2017), with permission from Elsevier.
SJLIFE cohort study investigators compared the cumulative burden of chronic health conditions among 4,612 adolescent and young adult survivors at the ages of 18 years (the time of transition from pediatric to adult health care systems) and 26 years (the time of transition from family to individual health insurance plans) with that of 625 controls.[20]
- Survivors at the age of 18 years experienced an average of 22.3 disabling conditions per 100 individuals versus 3.5 in controls, and 128.7 lower-severity conditions (at risk of progressing to higher-grade disabling conditions) versus 12.4 in controls.
- Survivors at the age of 26 years experienced an average of 40.3 disabling conditions per 100 individuals versus 5.7 in controls, and 240.5 lower-severity conditions versus 51.3 in controls.
- The cumulative burden of disabling, disease-specific conditions at the ages of 18 and 26 years was most notable for survivors of bone tumors (musculoskeletal: 99.9 and 121.70, respectively), soft tissue sarcomas (musculoskeletal: 49.5 and 54.1, respectively), and central nervous system (CNS) tumors (neurological: 24.7 and 36.8, respectively).
- The cumulative burden of lower-severity conditions (potentially amenable to intervention) at the ages of 18 and 26 years was most notable for neurological conditions across most cancer subgroups, with the highest cumulative burden in CNS tumor survivors (95.2 and 162.3, respectively).
- These findings highlight the importance of optimizing access to health care and health insurance as survivors age and can no longer participate in pediatric health care systems.
The variability in prevalence is related to differences in the following:
- Age and follow-up time of the cohorts studied.
- Methods and consistency of assessment (e.g., self-reported vs. risk-based medical evaluations).
- Treatment intensity and treatment era.
Childhood Cancer Survivor Study (CCSS) investigators demonstrated that the elevated risk of morbidity and mortality among aging survivors in the cohort increases beyond the fourth decade of life. By age 50 years, the cumulative incidence of a self-reported severe, disabling, life-threatening, or fatal health condition was 53.6% among survivors, compared with 19.8% among a sibling control group. Among survivors who reached age 35 years without a previous severe, disabling, life-threatening, or fatal health condition, 25.9% experienced a new grade 3 to grade 5 health condition within 10 years, compared with 6.0% of healthy siblings.[4]
The presence of serious, disabling, and life-threatening chronic health conditions adversely affects the health status of aging survivors. The greatest impact is on functional impairment and activity limitations. Predictably, chronic health conditions have been reported to contribute to a higher prevalence of emotional distress symptoms in adult survivors than in population controls.[21] Female survivors demonstrate a steeper trajectory of age-dependent decline in health status than do male survivors.[22] The even-higher prevalence of late effects among cohorts evaluated by clinical assessments is related to the subclinical and undiagnosed conditions detected by screening and surveillance measures.[7]
CCSS investigators also evaluated the impact of race and ethnicity on late outcomes. The study compared late mortality, subsequent neoplasms, and chronic health conditions in Hispanic (n = 750) and non-Hispanic Black (n = 694) participants with those in non-Hispanic White participants (n = 12,397).[23] The following results were observed:
- Cancer treatment did not account for disparities in mortality, chronic health conditions, or subsequent neoplasms observed among the groups.
- Differences in socioeconomic status and cardiovascular risk factors affected risk. All-cause mortality was higher among non-Hispanic Black participants than among other groups, but this difference disappeared after adjustment for socioeconomic status.
- Risk of developing diabetes was elevated among racial and ethnic minority groups even after adjustment for socioeconomic and obesity status.
- Non-Hispanic Black patients had a higher likelihood of reporting cardiac conditions, but this risk diminished after adjusting for cardiovascular risk factors.
- Nonmelanoma skin cancer was not reported by non-Hispanic Black participants, a finding that has been replicated by other studies.[24] Hispanic participants had a lower risk of nonmelanoma skin cancer than non-Hispanic White participants.
Recognition of late effects, concurrent with advances in cancer biology, radiological sciences, and supportive care, has resulted in a change in the prevalence and spectrum of treatment effects. In an effort to reduce and prevent late effects, contemporary therapy for most pediatric malignancies has evolved to a risk-adapted approach that is assigned on the basis of a variety of clinical, biological, and sometimes genetic factors.
The CCSS reported that with decreased cumulative dose and frequency of therapeutic radiation from 1970 to 1999, survivors have experienced a significant decrease in risk of subsequent neoplasms.[25]
- With the exception of survivors requiring intensive multimodality therapy for refractory/relapsed malignancies, life-threatening treatment effects are relatively uncommon after contemporary therapy in early follow-up (up to 10 years after diagnosis).
- However, survivors still frequently experience life-altering morbidity related to effects of cancer treatment on endocrine, reproductive, musculoskeletal, and neurological function.
A CCSS investigation examined temporal patterns in the cumulative incidence of severe to fatal chronic health conditions among survivors treated from 1970 to 1999.[26]
- The 20-year cumulative incidence of at least one grade 3 to 5 chronic condition decreased significantly, from 33.2% for survivors diagnosed between 1970 and 1979, to 29.3% for those diagnosed between 1980 and 1989, to 27.5% for those diagnosed between 1990 and 1999, compared with a 4.6% incidence in a sibling cohort.
- The overall decrease in incidence of chronic conditions across the three treatment decades was, in part, because of a substantial reduction of endocrinopathies, subsequent malignant neoplasms (SMNs), musculoskeletal conditions, and gastrointestinal conditions, whereas the cumulative incidence of hearing loss increased during this time.
- Declines in morbidity were not uniform across the diagnosis groups or condition types because of differences in treatment and survival patterns over time. For more information, see Figure 2.
- Despite declines in chronic health conditions over time, self-reported health status has not improved in more recent treatment eras. This finding may be because of the survival of children with higher-risk disease who would have previously died of cancer, or an enhanced awareness of and surveillance for late effects among more recently treated survivors.[27]
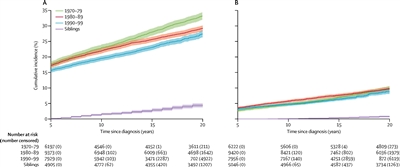
Figure 2. Cumulative incidence of grade 3–5 chronic health conditions in 5-year survivors of childhood cancer by diagnosis decade and siblings. (A) Cumulative incidence of a first grade 3–5 condition. (B) Cumulative incidence of two or more grade 3–5 conditions. The shaded area represents the 95% confidence interval (CI). The number of participants at risk (number censored) at each 5-year interval post-diagnosis is listed below the x-axis. The number censored does not include those who experienced a competing risk event (death from a cause other than a grade 5 chronic condition). Reprinted from The Lancet Oncology, Volume 19, Issue 12, Todd M Gibson, Sogol Mostoufi-Moab, Kayla L Stratton, Wendy M Leisenring, Dana Barnea, Eric J Chow, Sarah S Donaldson, Rebecca M Howell, Melissa M Hudson, Anita Mahajan, Paul C Nathan, Kirsten K Ness, Charles A Sklar, Emily S Tonorezos, Christopher B Weldon, Elizabeth M Wells, Yutaka Yasui, Gregory T Armstrong, Leslie L Robinson, Kevin C Oeffinger, Temporal patterns in the risk of chronic health conditions in survivors of childhood cancer diagnosed 1970–99: a report from the Childhood Cancer Survivor Study cohort. Pages 1590-1601, Copyright (2018), with permission from Elsevier.
Mortality
Late effects also contribute to an excess risk of premature death among long-term survivors of childhood cancer, as observed in the following studies:
- Several studies of large cohorts of survivors have reported early mortality among individuals treated for childhood cancer, compared with age- and sex-matched general population controls. Relapsed/refractory primary cancer remains the most frequent cause of death, followed by excess cause-specific mortality from subsequent primary cancers, and cardiac and pulmonary toxicity.[28,29,30,31,32,33]
- A CCSS study evaluated specific health-related causes of late mortality and excess deaths, compared with the general U.S. population to identify targets to reduce future risk.[33]
- At a median follow-up of 29 years from diagnosis, the 40-year cumulative all-cause mortality rate was 23.3%, with 51.2% of deaths attributed to health-related causes.
- Survivors who were 40 or more years from diagnosis experienced 131 excess health-related deaths per 10,000 person-years (95% confidence interval [CI], 111–163). Excess deaths were most commonly related to cancer (absolute excess risk per 10,000 person-years, 54; 95% CI, 41–68), heart disease (27; 18–38), and cerebrovascular disease (10; 5–17).
- Healthy lifestyle (assessed by smoking status, alcohol consumption, physical activity, body mass index, and absence of hypertension and diabetes) were each associated with a 20% to 30% reduction in health-related mortality, independent of other factors.
- An analysis of the CCSS and Surveillance, Epidemiology, and End Results (SEER) Program data evaluated conditional survival. The study demonstrated a subsequent 5-year survival rate of 92% or higher among most diagnoses at 5 years, 10 years, 15 years, and 20 years. Among those who had survived at least 5 years from diagnosis, the probability of all-cause mortality in the next 10 years was 8.8% in the CCSS and 10.6% in the SEER study, with neoplasms accounting for cause of death in approximately 75% of survivors.[34]
Despite high premature morbidity rates, overall mortality has decreased over time.[28,30,31,35,36]
CCSS investigators evaluated all-cause and health-related late mortality (including late effects of cancer therapy), SMNs, chronic health conditions, and neurocognitive outcomes among 6,148 survivors of childhood acute lymphoblastic leukemia (median age, 27.9 years; range, 5.9–61.9 years) diagnosed between 1970 and 1999.[37]
- Overall, the 20-year all-cause late mortality rate was 6.6%.
- Compared with participants who were treated in the 1970s, patients who were treated with risk-stratified regimens in the 1990s experienced lower health-related late mortality (rate ratio: 1990s standard risk, 0.2; 1990s high risk, 0.3), which was comparable to the U.S. population (standardized mortality ratio [SMR]: 1990s standard risk, 1.3; 1990s high risk, 1.7).
The risk of late mortality and serious chronic health conditions have decreased over time among survivors of acute myeloid leukemia (AML). CCSS investigators evaluated the long-term morbidity, mortality, and health status of more than 800 5-year survivors of childhood AML based on treatment and treatment era. Survivors were compared by treatment group (hematopoietic stem cell transplant [HSCT]); chemotherapy with cranial radiation [CRT]; chemotherapy only) and decade of diagnosis.[38]
- Among 856 survivors, the 20-year late mortality cumulative incidence was highest after HSCT (13.9%; chemotherapy with CRT, 7.6%; chemotherapy only, 5.1%).
- Mortality cumulative incidence decreased for survivors of HSCT diagnosed in the 1990s (8.5%) compared with the 1970s (38.9%), as did standardized mortality rates.
- Self-reported health status was good to excellent for 88.2% of childhood AML survivors, regardless of treatment.
- Most survivors did not experience any grade 3 to 5 chronic health conditions after 20 years (HSCT, 45.8%; chemotherapy with CRT, 23.7%; chemotherapy only, 27.0%).
- A temporal reduction in chronic health conditions cumulative incidence was seen after HSCT (1970s, 76.1%; 1990s, 38.3%; P = .02), mirroring a reduction in total-body irradiation use.
Population-based data from a state cancer registry was used to evaluate differences in survival and long-term outcomes by race and ethnicity among 4,222 children diagnosed with cancer between 1987 and 2012.[12]
- Compared with non-Hispanic White children, hospitalization was 70% (hazard ratio [HR], 1.7) more common 5 or more years after diagnosis for American Indian and Alaskan Native children and 50% (HR, 1.5) more common for Black children.
- Among survivors at 5 or more years from diagnosis, 2.3-fold to 3.6-fold statistically significant relative increases were observed for hospitalizations for specific conditions for American Indian and Alaskan Native children (HR, 2.3 for infection-related conditions; HR, 3.0 for hematologic-related conditions; HR, 2.6 for digestive-related conditions). The greatest increases were noted for mental health–related conditions (HR, 3.6), a pattern also noted for Black children (HR, 2.5).
An SJLIFE cohort study explored associations between modifiable chronic health conditions and late mortality within the context of social determinants of health.[39]
- Among 9,440 5-year childhood cancer survivors included in the analysis (median age at last follow-up, 27.5 years; median follow-up, 18.8 years), all-cause mortality (SMR, 7.6; 95% CI, 7.2–8.1) and health-related late mortality (SMR, 7.6; 95% CI, 7.0–8.2) was significantly higher than expected for U.S. mortality rates.
- Among 3,407 adult participants who completed an on-campus assessment (median age at assessment, 35.4 years; median follow-up, 27.3 years), significant increases in late all-cause and health-related deaths were associated with the number of modifiable chronic health conditions, living in a U.S. census block associated with a high area deprivation index, and frailty.
- Specific associations for excess health-related mortality included: one grade 2 modifiable chronic health condition (rate ratio [RR], 2.2; 95% CI, 1.1–4.4), two grade 2 modifiable chronic health conditions (RR, 2.5; 95% CI, 1.2–5.2), three grade 2 modifiable chronic health conditions (RR, 4.0; 95% CI, 1.9–8.4), area deprivation index in 51st to 80th percentile (RR, 9.2; 95% CI, 1.2–69.7), area deprivation index in 81st to 100th percentile (RR, 16.2; 95% CI, 2.1–123.7), and frailty (RR, 2.3; 95% CI, 1.2–4.1).
The CCSS and an SJLIFE cohort study investigated the contribution of cancer-predisposing variants to the risk of SMN-related late mortality (5 years or more after diagnosis).[40]
- Among 12,469 participants (6,172 male and 6,297 female), including 4,402 from the SJLIFE cohort (median follow-up time since collection of first biospecimen, 7.4 years) and 8,067 from the CCSS cohort (median follow-up time since collection of the first biospecimen, 12.6 years), 641 (5.1%) carried cancer-predisposing variants.
- Cancer-predisposing variants were significantly associated with an increased severity of SMNs (common terminology criteria for adverse events grade ≥4 vs. grade <4: odds ratio [OR], 2.15; 95% CI, 1.18–4.19).
- SMN-related deaths occurred in 263 participants (2.1%), and other-cause deaths occurred in 426 survivors (3.4%).
- At 10 years after the first biospecimen collection, the cumulative SMN-related mortality rate in carriers of cancer-predisposing variants was 3.7% (95% CI, 1.2%–8.5%) in SJLIFE and 6.9% (4.1%–10.7%) in CCSS. In comparison, the cumulative SMN-related mortality rate in noncarriers was 1.5% (1.0%–2.1%) in SJLIFE and 2.1% (1.7%–2.5%) in CCSS.
- Carrying a cancer-predisposing variant was associated with an increased risk of SMN-related mortality (SJLIFE: HR, 3.40; 95% CI, 1.37–8.43; CCSS: HR, 3.58; 95% CI, 2.27–5.63).
Survivors of adolescent and young adult (AYA) cancers
Little information is available on late mortality among survivors of AYA cancer.[41,42,43,44]
- Using SEER data, conditional relative survival up to 25 years after diagnosis was studied in a cohort of AYA patients (N = 205,954) diagnosed with a first malignant cancer (thyroid, melanoma, testicular, breast, lymphoma, leukemia, and CNS tumors).[41]
- For all cancer types combined, among individuals who survived up to 5 years, the subsequent 5-year relative survival rate exceeded 95% by 7 years after diagnosis.
- Most AYA cancer patients who survived at least 7 years after diagnosis experienced little difference in survival compared with the general population.
- For specific cancer types, including CNS tumors, female breast cancer, Hodgkin lymphoma, and leukemia, evidence of excess mortality risk persisted, or re-emerged, more than 10 years after a cancer diagnosis.
- Conditional relative survival was lowest for AYA patients with CNS tumors, although patients aged 15 to 29 years demonstrated a higher survival rate than did patients aged 30 to 39 years at the time of diagnosis of their CNS tumors.
- A separate analysis of 5-year survivors of AYA cancer (aged 15–39 years at diagnosis), also using SEER data (N = 282,969), demonstrated the following:[42]
- The 10-year all-cause mortality rate decreased from 8.3% for those diagnosed between 1975 and 1984 to 5.4% for those diagnosed between 2005 and 2011.
- The decrease in mortality primarily resulted from fewer deaths from the initial cancer.
- CCSS investigators compared chronic health conditions and all-cause and cause-specific mortality among 5,804 survivors of early-AYA cancer survivors (cancer diagnosis, age 15–20 years; median age, 42 years) and 5,804 childhood cancer survivors (cancer diagnosis, age <15 years; median age, 34 years) matched on primary cancer diagnosis.[43]
- The SMR was 5.9 (95% CI, 5.5–6.2) for early-AYA survivors and 6.2 (95% CI, 5.8–6.6) for younger childhood cancer survivors, compared with the general population.
- Early-AYA survivors had lower SMRs for death from health-related causes than did childhood cancer survivors (SMR, 4.8 [95% CI, 4.4–5.1] vs. 6.8 [95% CI, 6.2–7.4]), which was primarily evident more than 20 years after cancer diagnosis.
- Early-AYA and childhood cancer survivors were at greater risk of developing severe and disabling, life-threatening, or fatal (grades 3–5) health conditions than were siblings of the same age (HR, 4.2 [95% CI, 3.7–4.8] for early-AYA and 5.6 [95% CI, 4.9–6.3] for childhood cancer survivors), although the risk was lower for early-AYA survivors than for childhood cancer survivors.
- In a retrospective, population-based cohort study from Kaiser Permanente, cause-specific mortality in 2-year survivors (N = 10,574) of AYA cancers (patients aged 13–39 years who were diagnosed between 1990 and 2012) was examined and compared with individuals without cancer.[45]
- AYA cancer survivors were at a 10.4-fold increased risk of death compared with the matched noncancer cohort, and this risk remained elevated at more than 20 years after diagnosis (incidence rate ratio [IRR], 2.9).
- Beginning at 15 years after diagnosis, the incidence of second cancer–related mortality exceeded the rate of recurrence-related mortality.
- Mortality risk of suicide was doubled in AYA cancer survivors compared with the noncancer cohort.
- Chronic comorbidities were investigated in a retrospective, population-based cohort study of 6,778 2-year AYA cancer survivors diagnosed and monitored at Kaiser Permanente.[46]
- Approximately 17% of the survivors developed more than one comorbidity. The most common comorbidities were dyslipidemia (22 per 1,000 person-years), hypertension (16 per 1,000 person-years), diabetes (10 per 1,000 person-years), thyroid disorders (9 per 1,000 person-years), and severe depression or anxiety (8 per 1,000 person-years).
- IRRs were higher in survivors than in controls without a history of cancer for avascular necrosis (IRR, 8.25), followed by osteoporosis (IRR, 5.75), joint replacement (IRR, 3.89), stroke (IRR, 3.19), premature ovarian failure (IRR, 2.87), and cardiomyopathy or heart failure (IRR, 2.64).
- For survivors of AYA cancer, the prevalence of multiple comorbidities approached 40% at 10 years after index date (a 2-year time point from diagnosis), compared with 20% for those without cancer (P < .001).
Monitoring for Late Effects
Recognition of both acute and late modality–specific toxicity has motivated investigations evaluating the pathophysiology and prognostic factors for cancer treatment–related effects. Consequently, the results of late effects research have played an important role in the following areas:
- Changing pediatric cancer therapeutic approaches to reduce treatment-related mortality among survivors treated in more recent eras.[47]
- The development of risk counseling and health screening recommendations for long-term survivors by identifying the clinical and treatment characteristics of those at highest risk of therapy-related complications.[48]
The common late effects of pediatric cancer encompass several broad domains, including the following:
- Growth and development.
- Organ function.
- Reproductive capacity and health of offspring.
- Secondary carcinogenesis.
- Psychosocial sequelae related to the primary cancer, its treatment, or maladjustment associated with the cancer experience.
Late sequelae of therapy for childhood cancer can be anticipated based on therapeutic exposures, but the magnitude of risk and the manifestations in an individual patient are influenced by numerous factors. Multiple factors should be considered in the risk assessment for a given late effect (see Figure 3).[49]
Cancer-related factors:
- Organs or tissues affected by the cancer.
- Direct tissue effects.
- Cancer-induced organ dysfunction or other tissue effects.
Treatment-related factors:
- Radiation therapy: Total dose, fraction size, organ or tissue volume exposed.
- Chemotherapy: Agent type, dose-intensity, cumulative dose, schedule.
- Surgery: Technique, site, consequential organ dysfunction.
- HSCT.
- Combined-modality effects (therapeutic interactions).
- Blood product transfusion.
- Chronic graft-versus-host disease.
Host-related factors:
- Sex.
- Genetic predisposition.
- Premorbid, comorbid, posttreatment health states and exposures.
- Developmental status (age).
- Time from diagnosis/therapy.
- Inherent tissue sensitivities and capacity for normal tissue repair.
- Hormonal milieu.
- Socioeconomic status.
- Health habits.
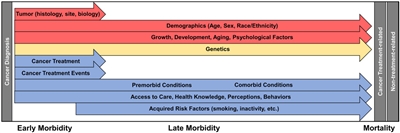
Figure 3. Factors influencing morbidity and mortality of the childhood cancer survivor. Each arrow indicates a different factor affecting morbidity and mortality that exerts its effect along a continuum of care. Note that all effectors can begin exerting influence on morbidity during the period of cancer-directed therapy. Factors are separated into those that cannot be modified (red), those for which future interventions are plausible (yellow), and those for which there are known targets for interventions or areas in which therapy and surveillance have already been modified (blue). Reprinted from CA: A Cancer Journal for Clinicians, Volume 68, Issue 2, Dixon SB, Bjornard KL, Alberts NM, et al., Factors influencing risk-based care of the childhood cancer survivor in the 21st century, Pages 133–152, Copyright © 2018 American Cancer Society, with permission from John Wiley and Sons.
Resources to Support Survivor Care
Risk-based screening
The need for long-term follow-up of childhood cancer survivors is supported by the American Society of Pediatric Hematology/Oncology, the International Society of Pediatric Oncology, the American Academy of Pediatrics, the Children's Oncology Group (COG), and the Institute of Medicine. A risk-based medical follow-up is recommended, which includes a systematic plan for lifelong screening, surveillance, and prevention that incorporates risk estimates based on the following:[49]
- Previous cancer.
- Cancer therapy.
- Genetic predisposition.
- Lifestyle behaviors.
- Comorbid conditions.
- Sex.
Part of long-term follow-up also focuses on appropriate screening of educational and vocational progress. Specific treatments for childhood cancer, especially those that directly impact nervous system structures, may result in sensory, motor, and neurocognitive deficits that may have adverse effects on functional status, educational attainment, and future vocational opportunities. In support of this, a CCSS investigation observed the following:[50]
- Treatment with cranial radiation doses of 25 Gy or higher was associated with higher odds of unemployment (health related: OR, 3.47; 95% CI, 2.54–4.74; seeking work: OR, 1.77; 95% CI, 1.15–2.71).
- Unemployed survivors reported higher levels of poor physical functioning than employed survivors, had lower education and income, and were more likely to be publicly insured than unemployed siblings.
These data emphasize the importance of facilitating survivor access to individualized education services, which has been demonstrated to have a positive impact on education achievement.[51] These services may in turn enhance vocational opportunities.
In addition to risk-based screening for medical late effects, the impact of health behaviors on cancer-related health risks is also emphasized. Health-promoting behaviors are stressed for survivors of childhood cancer. Educational efforts focused on healthy lifestyle behaviors include the following:
- Abstinence from smoking, excess alcohol use, and illicit drug use to reduce the risk of organ toxicity and, potentially, subsequent neoplasms.
- Healthy dietary practices (e.g., a diet rich in plant foods and moderate in animal foods) [52] and active lifestyle to reduce treatment-related metabolic and cardiovascular complications.
- Regular physical activity to reduce neurocognitive problems and enhance psychological outcomes.[53,54]
- Survivors who engaged in consistent physical activity over time had fewer neurocognitive problems, including difficulties with task efficiency, emotional regulation, organization, and memory. They also experienced larger neurocognitive improvements, compared with those who had inconsistent activity levels.[53]
- Vigorous exercise in survivors has been associated with a lower prevalence of depression and somatization, as well as less impairment in physical functioning, general health and vitality, emotional role limitations, and mental health quality-of-life domains.[54]
Proactively addressing unhealthy and risky behaviors is pertinent because several research investigations confirm that long-term survivors use tobacco and alcohol and have inactive lifestyles despite their increased risk of cardiac, pulmonary, and metabolic late effects.[55,56,57]
Access to risk-based survivor care
Most childhood cancer survivors do not receive recommended risk-based care. The CCSS observed the following:
- 92.8% of survivors reported receiving some form of medical care in the previous year.[58]
- Nearly 40% reported receiving care that focused on their previous cancer (survivor-focused care).[58]
- Surveillance for new cases of cancer was very low in survivors at the highest risk of colon, breast, or skin cancer, suggesting that survivors and their physicians need education about the risk of subsequent neoplasms and recommended surveillance.[59]
- Sociodemographic factors have been linked to declining rates of follow-up care over time from diagnosis. CCSS participants who were male, had a household income of less than $20,000 per year, and had lower educational attainment (high school education or less) were more likely to report no care at their most recent follow-up survey. This trend is concerning because the prevalence of chronic health conditions increases with longer elapsed time from cancer diagnosis in adults treated for cancer during childhood.[60]
- A study that included 975 adult survivors of childhood cancer identified factors associated with attending the recommended risk-based, cancer-related medical visits. The relative risk of having a cancer-related visit was higher among survivors who:[61]
- Assigned a greater importance to these visits.
- Perceived a greater susceptibility to health problems.
- Had experienced a cancer-related chronic health problem that was moderate to life-threatening.
- Were seeing a primary care provider for a cancer-related problem.
- Had received a cancer treatment care plan.
- Expressed greater confidence in physicians' abilities to address questions and concerns.
Access to health insurance appears to play an important role in risk-based survivor care.[62,63] Lack of access to health insurance affects the following:
- Cancer-related visits. In the CCSS, uninsured survivors were less likely than those privately insured to report a cancer-related visit (adjusted relative risk, 0.83; 95% CI, 0.75–0.91) or a cancer center visit (adjusted relative risk, 0.83; 95% CI, 0.71–0.98). Uninsured survivors had lower levels of utilization in all measures of care than privately insured survivors. In contrast, publicly insured survivors were more likely to report a cancer-related visit (adjusted relative risk, 1.22; 95% CI, 1.11–1.35) or a cancer center visit (adjusted relative risk, 1.41; 95% CI, 1.18–1.70) than were privately insured survivors.[62]
- Health care outcomes. In a study comparing health care outcomes for long-term AYA cancer survivors with young adults who have no cancer history, the proportion of uninsured survivors did not differ between the two groups.[64]
- Financial burden. Subgroups of adult survivors of childhood cancer may be at additional risk of health care barriers due to financial hardship. Younger survivors (aged 20–29 years), females, non-White survivors, and survivors reporting poorer health faced more cost barriers, which may inhibit the early detection of late effects.[64] Survivors are more likely than their siblings to forego needed medical care related to financial challenges.[65]
Overall, lack of health insurance—related to health issues, unemployment, and other societal factors—remains a significant concern for survivors of childhood cancer.[66,67] Legislation, including the Health Insurance Portability and Accountability Act (HIPAA),[68,69] has improved access and retention of health insurance among survivors, although the quality and limitations associated with these policies have not been well studied.
Transition to Survivor Care
Long-term follow-up programs
Transition of care from the pediatric to adult health care setting is necessary for most childhood cancer survivors in the United States.
When available, multidisciplinary long-term follow-up programs in the pediatric cancer center work collaboratively with community physicians to provide care for childhood cancer survivors. This type of shared care has been proposed as the optimal model to facilitate coordination between the cancer center oncology team and community physician groups providing survivor care.[70]
An essential service of long-term follow-up programs is the organization of an individualized survivorship care plan that includes the following:
- Details about therapeutic interventions undertaken for childhood cancer and their potential health risks (e.g., chemotherapy type and cumulative dose, radiation treatment fields and dose, surgical procedures, blood product transfusions, and HSCT).
- Personalized health screening recommendations.
- Information about lifestyle factors that modify risks.
A CCSS investigation that evaluated perceptions of future health and cancer risk highlighted the importance of continuing education of survivors during long-term follow-up evaluations. A substantial subgroup of adult survivors reported a lack of concern about future health (24%) and subsequent cancer risks (35%), even after exposure to treatments associated with increased risks. These findings present concerns that survivors may be less likely to engage in beneficial screenings and risk-reduction activities.[71]
The CCSS evaluated the surveillance and screening practices of 11,337 childhood cancer survivors. They found that fewer than half of high-risk survivors at increased risk of developing SMNs or cardiac dysfunction received the recommended surveillance, which likely exposes them to preventable morbidity and mortality.[59]
- 27% of survivors and 20% of primary care providers (PCP) had a survivorship care plan. Survivors treated after 1990 were more likely to have a survivorship care plan.
- Survivorship care plan possession by high-risk survivors was associated with increased adherence to COG-recommended breast (22% vs. 8%), skin (35% vs. 23%), and cardiac (67% vs. 33%) surveillance. PCP survivorship care plan possession was associated with increased adherence to skin surveillance (40% vs. 23%).
- Among high-risk survivors, adherence increased for colorectal (14% to 41%, P < .001) and cardiac (22% to 38%, P < .001) surveillance and decreased for breast surveillance (38% to 13%, P < .001) between 2007 and 2016.
- For average-risk survivors, better adherence to American Cancer Society recommendations for breast (57%), cervical (84%), and colorectal (69%) screening was observed than with COG recommendations. PCP survivorship care plan possession was associated with increased adherence to breast and colorectal screening. Survivors were less adherent to breast screening than the general population and less adherent to cervical screening than siblings.
For survivors who have not been provided with this information, the COG offers a template that can be used by survivors to organize a personal treatment summary. For more information, see the COG Survivorship Guidelines, Appendix 1.
COG long-term follow-up guidelines for childhood and AYA cancer survivors
To facilitate survivor and provider access to succinct information to guide risk-based care, COG investigators have organized a compendium of exposure- and risk-based health surveillance recommendations, with the goal of standardizing the care of childhood cancer survivors.[72]
The compendium of resources includes the following:
- Long-Term Follow-Up Guidelines. COG Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers are appropriate for asymptomatic survivors presenting for routine exposure-based medical evaluation 2 or more years after completion of therapy.
- Health Links. Patient education materials called Health Links provide detailed information on guideline-specific topics to enhance health maintenance and promotion among this population of cancer survivors.[73]
Information concerning late effects is summarized in tables throughout this summary.
Several groups have undertaken research to evaluate the yield from risk-based screening as recommended by the COG and other pediatric oncology cooperative groups.[7,74,75] Pertinent considerations in interpreting the results of these studies include the following:
- Variability in the cohort's age at treatment.
- Age at screening.
- Time from cancer treatment.
- Participation bias.
Collectively, these studies demonstrate that screening identifies a substantial proportion of individuals with previously unrecognized, treatment-related health complications of varying degrees of severity. Study results have also identified low-yield evaluations that have encouraged revisions of screening recommendations. Ongoing research is evaluating the cost effectiveness of screening in the context of consideration of benefits, risks, and harms.
References:
- National Cancer Institute: NCCR*Explorer: An interactive website for NCCR cancer statistics. Bethesda, MD: National Cancer Institute. Available online. Last accessed February 25, 2025.
- Lorenzi MF, Xie L, Rogers PC, et al.: Hospital-related morbidity among childhood cancer survivors in British Columbia, Canada: report of the childhood, adolescent, young adult cancer survivors (CAYACS) program. Int J Cancer 128 (7): 1624-31, 2011.
- Rebholz CE, Reulen RC, Toogood AA, et al.: Health care use of long-term survivors of childhood cancer: the British Childhood Cancer Survivor Study. J Clin Oncol 29 (31): 4181-8, 2011.
- Armstrong GT, Kawashima T, Leisenring W, et al.: Aging and risk of severe, disabling, life-threatening, and fatal events in the childhood cancer survivor study. J Clin Oncol 32 (12): 1218-27, 2014.
- Teepen JC, Kok JL, Feijen EAM, et al.: Questionnaire- and linkage-based outcomes in Dutch childhood cancer survivors: Methodology of the DCCSS LATER study part 1. Cancer Med 12 (6): 7588-7602, 2023.
- Geenen MM, Cardous-Ubbink MC, Kremer LC, et al.: Medical assessment of adverse health outcomes in long-term survivors of childhood cancer. JAMA 297 (24): 2705-15, 2007.
- Hudson MM, Ness KK, Gurney JG, et al.: Clinical ascertainment of health outcomes among adults treated for childhood cancer. JAMA 309 (22): 2371-81, 2013.
- Feijen EAM, Teepen JC, van Dulmen-den Broeder E, et al.: Clinical evaluation of late outcomes in Dutch childhood cancer survivors: Methodology of the DCCSS LATER 2 study. Pediatr Blood Cancer 70 (5): e30212, 2023.
- Kurt BA, Nolan VG, Ness KK, et al.: Hospitalization rates among survivors of childhood cancer in the Childhood Cancer Survivor Study cohort. Pediatr Blood Cancer 59 (1): 126-32, 2012.
- Zhang Y, Lorenzi MF, Goddard K, et al.: Late morbidity leading to hospitalization among 5-year survivors of young adult cancer: a report of the childhood, adolescent and young adult cancer survivors research program. Int J Cancer 134 (5): 1174-82, 2014.
- Sørensen GV, Winther JF, de Fine Licht S, et al.: Long-Term Risk of Hospitalization Among Five-Year Survivors of Childhood Leukemia in the Nordic Countries. J Natl Cancer Inst 111 (9): 943-951, 2019.
- Emerson MA, Olshan AF, Chow EJ, et al.: Hospitalization and Mortality Outcomes Among Childhood Cancer Survivors by Race, Ethnicity, and Time Since Diagnosis. JAMA Netw Open 5 (6): e2219122, 2022.
- Streefkerk N, Tissing WJE, Korevaar JC, et al.: A detailed insight in the high risks of hospitalizations in long-term childhood cancer survivors-A Dutch LATER linkage study. PLoS One 15 (5): e0232708, 2020.
- Berbis J, Michel G, Chastagner P, et al.: A French cohort of childhood leukemia survivors: impact of hematopoietic stem cell transplantation on health status and quality of life. Biol Blood Marrow Transplant 19 (7): 1065-72, 2013.
- Phillips SM, Padgett LS, Leisenring WM, et al.: Survivors of childhood cancer in the United States: prevalence and burden of morbidity. Cancer Epidemiol Biomarkers Prev 24 (4): 653-63, 2015.
- Bhakta N, Liu Q, Ness KK, et al.: The cumulative burden of surviving childhood cancer: an initial report from the St Jude Lifetime Cohort Study (SJLIFE). Lancet 390 (10112): 2569-2582, 2017.
- Salloum R, Chen Y, Yasui Y, et al.: Late Morbidity and Mortality Among Medulloblastoma Survivors Diagnosed Across Three Decades: A Report From the Childhood Cancer Survivor Study. J Clin Oncol 37 (9): 731-740, 2019.
- Streefkerk N, Teepen JC, Feijen EAM, et al.: The cumulative burden of self-reported, clinically relevant outcomes in long-term childhood cancer survivors and implications for survivorship care: A DCCSS LATER study. Cancer 130 (8): 1349-1358, 2024.
- Esbenshade AJ, Lu L, Friedman DL, et al.: Accumulation of Chronic Disease Among Survivors of Childhood Cancer Predicts Early Mortality. J Clin Oncol 41 (20): 3629-3641, 2023.
- Ehrhardt MJ, Williams AM, Liu Q, et al.: Cumulative burden of chronic health conditions among adolescent and young adult survivors of childhood cancer: Identification of vulnerable groups at key medical transitions. Pediatr Blood Cancer 68 (6): e29030, 2021.
- Vuotto SC, Krull KR, Li C, et al.: Impact of chronic disease on emotional distress in adult survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. Cancer 123 (3): 521-528, 2017.
- Hudson MM, Oeffinger KC, Jones K, et al.: Age-dependent changes in health status in the Childhood Cancer Survivor cohort. J Clin Oncol 33 (5): 479-91, 2015.
- Liu Q, Leisenring WM, Ness KK, et al.: Racial/Ethnic Differences in Adverse Outcomes Among Childhood Cancer Survivors: The Childhood Cancer Survivor Study. J Clin Oncol 34 (14): 1634-43, 2016.
- Ehrhardt MJ, Bhakta N, Liu Q, et al.: Absence of Basal Cell Carcinoma in Irradiated Childhood Cancer Survivors of Black Race: A Report from the St. Jude Lifetime Cohort Study. Cancer Epidemiol Biomarkers Prev 25 (9): 1356-60, 2016.
- Turcotte LM, Liu Q, Yasui Y, et al.: Temporal Trends in Treatment and Subsequent Neoplasm Risk Among 5-Year Survivors of Childhood Cancer, 1970-2015. JAMA 317 (8): 814-824, 2017.
- Gibson TM, Mostoufi-Moab S, Stratton KL, et al.: Temporal patterns in the risk of chronic health conditions in survivors of childhood cancer diagnosed 1970-99: a report from the Childhood Cancer Survivor Study cohort. Lancet Oncol 19 (12): 1590-1601, 2018.
- Ness KK, Hudson MM, Jones KE, et al.: Effect of Temporal Changes in Therapeutic Exposure on Self-reported Health Status in Childhood Cancer Survivors. Ann Intern Med 166 (2): 89-98, 2017.
- Armstrong GT, Chen Y, Yasui Y, et al.: Reduction in Late Mortality among 5-Year Survivors of Childhood Cancer. N Engl J Med 374 (9): 833-42, 2016.
- Holmqvist AS, Chen Y, Wu J, et al.: Late mortality after autologous blood or marrow transplantation in childhood: a Blood or Marrow Transplant Survivor Study-2 report. Blood 131 (24): 2720-2729, 2018.
- Bagnasco F, Caruso S, Andreano A, et al.: Late mortality and causes of death among 5-year survivors of childhood cancer diagnosed in the period 1960-1999 and registered in the Italian Off-Therapy Registry. Eur J Cancer 110: 86-97, 2019.
- Byrne J, Schmidtmann I, Rashid H, et al.: Impact of era of diagnosis on cause-specific late mortality among 77 423 five-year European survivors of childhood and adolescent cancer: The PanCareSurFup consortium. Int J Cancer 150 (3): 406-419, 2022.
- Kilsdonk E, van Dulmen-den Broeder E, van Leeuwen FE, et al.: Late Mortality in Childhood Cancer Survivors according to Pediatric Cancer Diagnosis and Treatment Era in the Dutch LATER Cohort. Cancer Invest 40 (5): 413-424, 2022.
- Dixon SB, Liu Q, Chow EJ, et al.: Specific causes of excess late mortality and association with modifiable risk factors among survivors of childhood cancer: a report from the Childhood Cancer Survivor Study cohort. Lancet 401 (10386): 1447-1457, 2023.
- Mertens AC, Yong J, Dietz AC, et al.: Conditional survival in pediatric malignancies: analysis of data from the Childhood Cancer Survivor Study and the Surveillance, Epidemiology, and End Results Program. Cancer 121 (7): 1108-17, 2015.
- Fidler MM, Reulen RC, Winter DL, et al.: Long term cause specific mortality among 34 489 five year survivors of childhood cancer in Great Britain: population based cohort study. BMJ 354: i4351, 2016.
- Holmqvist AS, Chen Y, Wu J, et al.: Assessment of Late Mortality Risk After Allogeneic Blood or Marrow Transplantation Performed in Childhood. JAMA Oncol 4 (12): e182453, 2018.
- Dixon SB, Chen Y, Yasui Y, et al.: Reduced Morbidity and Mortality in Survivors of Childhood Acute Lymphoblastic Leukemia: A Report From the Childhood Cancer Survivor Study. J Clin Oncol 38 (29): 3418-3429, 2020.
- Turcotte LM, Whitton JA, Leisenring WM, et al.: Chronic conditions, late mortality, and health status after childhood AML: a Childhood Cancer Survivor Study report. Blood 141 (1): 90-101, 2023.
- Ehrhardt MJ, Liu Q, Dixon SB, et al.: Association of Modifiable Health Conditions and Social Determinants of Health With Late Mortality in Survivors of Childhood Cancer. JAMA Netw Open 6 (2): e2255395, 2023.
- Chen C, Qin N, Wang M, et al.: Cancer germline predisposing variants and late mortality from subsequent malignant neoplasms among long-term childhood cancer survivors: a report from the St Jude Lifetime Cohort and the Childhood Cancer Survivor Study. Lancet Oncol 24 (10): 1147-1156, 2023.
- Anderson C, Smitherman AB, Nichols HB: Conditional relative survival among long-term survivors of adolescent and young adult cancers. Cancer 124 (14): 3037-3043, 2018.
- Anderson C, Nichols HB: Trends in Late Mortality Among Adolescent and Young Adult Cancer Survivors. J Natl Cancer Inst 112 (10): 994-1002, 2020.
- Suh E, Stratton KL, Leisenring WM, et al.: Late mortality and chronic health conditions in long-term survivors of early-adolescent and young adult cancers: a retrospective cohort analysis from the Childhood Cancer Survivor Study. Lancet Oncol 21 (3): 421-435, 2020.
- Rossetti S, Juul SJ, Eriksson F, et al.: Long-term cause-specific mortality in adolescent and young adult Hodgkin lymphoma patients treated with contemporary regimens-A nationwide Danish cohort study. Br J Haematol 205 (4): 1374-1382, 2024.
- Armenian SH, Xu L, Cannavale KL, et al.: Cause-specific mortality in survivors of adolescent and young adult cancer. Cancer 126 (10): 2305-2316, 2020.
- Chao C, Bhatia S, Xu L, et al.: Chronic Comorbidities Among Survivors of Adolescent and Young Adult Cancer. J Clin Oncol 38 (27): 3161-3174, 2020.
- Hudson MM, Armenian SH, Armstrong GT, et al.: Optimization of Health and Extension of Lifespan Through Childhood Cancer Survivorship Research. J Clin Oncol 36 (21): 2133-2134, 2018.
- Kremer LC, Mulder RL, Oeffinger KC, et al.: A worldwide collaboration to harmonize guidelines for the long-term follow-up of childhood and young adult cancer survivors: a report from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Pediatr Blood Cancer 60 (4): 543-9, 2013.
- Dixon SB, Bjornard KL, Alberts NM, et al.: Factors influencing risk-based care of the childhood cancer survivor in the 21st century. CA Cancer J Clin 68 (2): 133-152, 2018.
- Kirchhoff AC, Leisenring W, Krull KR, et al.: Unemployment among adult survivors of childhood cancer: a report from the childhood cancer survivor study. Med Care 48 (11): 1015-25, 2010.
- Mitby PA, Robison LL, Whitton JA, et al.: Utilization of special education services and educational attainment among long-term survivors of childhood cancer: a report from the Childhood Cancer Survivor Study. Cancer 97 (4): 1115-26, 2003.
- Lan T, Wang M, Ehrhardt MJ, et al.: Adherence to healthy diet and risk of cardiovascular disease in adult survivors of childhood cancer in the St. Jude Lifetime Cohort: a cross-sectional study. BMC Med 21 (1): 242, 2023.
- Barlow-Krelina E, Chen Y, Yasui Y, et al.: Consistent Physical Activity and Future Neurocognitive Problems in Adult Survivors of Childhood Cancers: A Report From the Childhood Cancer Survivor Study. J Clin Oncol 38 (18): 2041-2052, 2020.
- Tonorezos ES, Ford JS, Wang L, et al.: Impact of exercise on psychological burden in adult survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. Cancer 125 (17): 3059-3067, 2019.
- Lown EA, Hijiya N, Zhang N, et al.: Patterns and predictors of clustered risky health behaviors among adult survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. Cancer 122 (17): 2747-56, 2016.
- Gibson TM, Liu W, Armstrong GT, et al.: Longitudinal smoking patterns in survivors of childhood cancer: An update from the Childhood Cancer Survivor Study. Cancer 121 (22): 4035-43, 2015.
- Devine KA, Mertens AC, Whitton JA, et al.: Factors associated with physical activity among adolescent and young adult survivors of early childhood cancer: A report from the childhood cancer survivor study (CCSS). Psychooncology 27 (2): 613-619, 2018.
- Mueller EL, Park ER, Kirchhoff AC, et al.: Insurance, chronic health conditions, and utilization of primary and specialty outpatient services: a Childhood Cancer Survivor Study report. J Cancer Surviv 12 (5): 639-646, 2018.
- Yan AP, Chen Y, Henderson TO, et al.: Adherence to Surveillance for Second Malignant Neoplasms and Cardiac Dysfunction in Childhood Cancer Survivors: A Childhood Cancer Survivor Study. J Clin Oncol 38 (15): 1711-1722, 2020.
- Casillas J, Oeffinger KC, Hudson MM, et al.: Identifying Predictors of Longitudinal Decline in the Level of Medical Care Received by Adult Survivors of Childhood Cancer: A Report from the Childhood Cancer Survivor Study. Health Serv Res 50 (4): 1021-42, 2015.
- Ford JS, Tonorezos ES, Mertens AC, et al.: Barriers and facilitators of risk-based health care for adult survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. Cancer 126 (3): 619-627, 2020.
- Casillas J, Castellino SM, Hudson MM, et al.: Impact of insurance type on survivor-focused and general preventive health care utilization in adult survivors of childhood cancer: the Childhood Cancer Survivor Study (CCSS). Cancer 117 (9): 1966-75, 2011.
- Keegan TH, Tao L, DeRouen MC, et al.: Medical care in adolescents and young adult cancer survivors: what are the biggest access-related barriers? J Cancer Surviv 8 (2): 282-92, 2014.
- Kirchhoff AC, Lyles CR, Fluchel M, et al.: Limitations in health care access and utilization among long-term survivors of adolescent and young adult cancer. Cancer 118 (23): 5964-72, 2012.
- Nathan PC, Huang IC, Chen Y, et al.: Financial Hardship in Adult Survivors of Childhood Cancer in the Era After Implementation of the Affordable Care Act: A Report From the Childhood Cancer Survivor Study. J Clin Oncol 41 (5): 1000-1010, 2023.
- Kirchhoff AC, Kuhlthau K, Pajolek H, et al.: Employer-sponsored health insurance coverage limitations: results from the Childhood Cancer Survivor Study. Support Care Cancer 21 (2): 377-83, 2013.
- Kuhlthau KA, Nipp RD, Shui A, et al.: Health insurance coverage, care accessibility and affordability for adult survivors of childhood cancer: a cross-sectional study of a nationally representative database. J Cancer Surviv 10 (6): 964-971, 2016.
- Park ER, Kirchhoff AC, Zallen JP, et al.: Childhood Cancer Survivor Study participants' perceptions and knowledge of health insurance coverage: implications for the Affordable Care Act. J Cancer Surviv 6 (3): 251-9, 2012.
- Warner EL, Park ER, Stroup A, et al.: Childhood cancer survivors' familiarity with and opinions of the Patient Protection and Affordable Care Act. J Oncol Pract 9 (5): 246-50, 2013.
- Jacobs LA, Shulman LN: Follow-up care of cancer survivors: challenges and solutions. Lancet Oncol 18 (1): e19-e29, 2017.
- Gibson TM, Li C, Armstrong GT, et al.: Perceptions of future health and cancer risk in adult survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. Cancer 124 (16): 3436-3444, 2018.
- Landier W, Bhatia S, Eshelman DA, et al.: Development of risk-based guidelines for pediatric cancer survivors: the Children's Oncology Group Long-Term Follow-Up Guidelines from the Children's Oncology Group Late Effects Committee and Nursing Discipline. J Clin Oncol 22 (24): 4979-90, 2004.
- Eshelman D, Landier W, Sweeney T, et al.: Facilitating care for childhood cancer survivors: integrating children's oncology group long-term follow-up guidelines and health links in clinical practice. J Pediatr Oncol Nurs 21 (5): 271-80, 2004 Sep-Oct.
- Landier W, Armenian SH, Lee J, et al.: Yield of screening for long-term complications using the children's oncology group long-term follow-up guidelines. J Clin Oncol 30 (35): 4401-8, 2012.
- Wasilewski-Masker K, Mertens AC, Patterson B, et al.: Severity of health conditions identified in a pediatric cancer survivor program. Pediatr Blood Cancer 54 (7): 976-82, 2010.
Subsequent Neoplasms
Subsequent neoplasms (SNs) are defined as histologically distinct neoplasms developing at least 2 months after completion of treatment for the primary malignancy. SNs may be benign or malignant. Childhood cancer survivors have increased risks of developing SNs that are multifactorial in etiology and vary according to the following:
- Host factors (e.g., genetics, immune function, hormone status).
- Primary cancer therapy.
- Environmental exposures.
- Lifestyle factors.
SNs are the leading cause of nonrelapse late mortality (standardized mortality ratio, 15.2; 95% confidence interval [CI], 13.9–16.6).[1] The Childhood Cancer Survivor Study (CCSS) reported the following 30-year cumulative incidence rates:[2]
- All SNs: 20.5% (95% CI, 19.1%–21.8%).
- Nonmelanoma skin cancer (NMSC): 9.1% (95% CI, 8.1%–10.1%).
- SNs with malignant histologies (excluding NMSC): 7.9% (95% CI, 7.2%–8.5%).
- Meningioma: 3.1% (95% CI, 2.5%–3.8%).
This represents a sixfold increased risk of SNs among cancer survivors, compared with the general population.[2]
Several studies have described the excess risk of SNs.[3,4]
Evidence (excess risk of SNs):
- A population-based study that leveraged registry data evaluated early second primary tumors occurring within 5 years of a first primary cancer diagnosed before age 15 years (1971–2010).[5]
- Early second primary tumors developed in 0.4% of cancer survivors, which is a sevenfold excess risk (standardized incidence ratio [SIR], 7.7; 95% CI, 6.7–8.9).
- Excess risk was higher among children diagnosed between 1981 and 1990 (SIR, 9.5; 95% CI, 7.1–12.5), compared with earlier or later decades (SIR, 6.5–7.5).
- Cancer predisposition syndromes were implicated in 21% of children with early second primary tumors and suspected in another 5%.
- An international case-control study pooled data for an analysis of meningioma risk after treatment for childhood cancer. The study evaluated the magnitude of radiation dose–response association, potential modifiers of radiation risks, and the role of chemotherapy.[6]
- Increasing radiation dose was associated with increased risk of meningioma (excess odds ratio [OR]/Gy, 1.44; 95% CI, 0.6–3.6), without evidence of departure from linearity.
- Exposure to radiation doses of 24 Gy or higher was associated with more than 30-fold higher odds of developing a meningioma (OR, 33.7; 95% CI, 14.1–80.3).
- Patients aged 10 years or older at treatment had a significantly lower radiation dose–response association compared with those treated before the age of 10 years (excess OR/Gy, 0.57; 95% CI, 0.18–1.91 vs. 2.20; 95% CI, 0.87–6.31).
- Treatment with methotrexate was associated with an increased risk of meningioma (OR, 3.43; 95% CI, 1.56–7.57), but without evidence of a dose-response association or interaction with radiation dose.
- Meningioma risk associated with radiation exposure remained significantly elevated 30 years after treatment (excess OR/Gy, 3.76; 95% CI, 0.77–29.15).
- A CCSS cohort reported on any new SN (including malignant neoplasms, NMSCs, benign meningiomas, and other benign neoplasms) occurring after age 40 years.[3]
- At the age of 55 years, the cumulative incidence of any new SN was 34.6%. The incidence of malignant SNs was 16.3%.
- Female sex and therapeutic radiation exposure were associated with an increased risk of developing SNs in multivariate analysis.
Prolonged follow-up has established that multiple SNs are common among aging childhood cancer survivors.[7,8]
- The CCSS also reported the following:[4]
- Individuals treated in more recent treatment eras experienced decreased risk of SNs (including subsequent malignancies, NMSCs, and benign meningiomas) compared with those treated earlier. This lower risk was attributed to decreased exposure to therapeutic radiation.
- However, individuals treated in the 1990s remain at increased risk of SNs compared with the general population.
- CCSS investigators evaluated morbidity and mortality associated with meningioma among 4,221 participants treated with cranial radiation therapy.[9]
- The cumulative incidence of subsequent meningioma by age 40 years was 5.6% in this group of patients, and the incidence was without demonstrable plateau.
- Risk factors for subsequent meningioma included female sex (hazard ratio [HR], 1.7; 95% CI, 1.2–2.3) and higher cranial radiation dose (HR, 2.6; 95% CI, 1.6–4.2 after 30 Gy or higher).
- Among survivors reporting meningiomas, the risk of neurological sequelae occurring 5 or more years after primary cancer diagnosis was increased for seizures (HR, 10.0; 95% CI, 7.0–15.3); auditory-vestibular-visual sensory deficits (HR, 2.3; 95% CI, 1.3–4.0); focal neurological dysfunction (HR, 4.9; 95% CI, 3.2–7.5); and severe headaches (HR, 3.2; 95% CI, 1.9–5.4).
- With a median follow-up of 72 months after meningioma diagnosis, 13% of the patients had died, with six deaths attributed to meningioma.
- Dutch Childhood Oncology Group (DCOG)–LATER investigators evaluated the cumulative meningioma incidence and performed excess relative risk modeling of benign meningiomas in childhood cancer patients.[10]
- Among 5,843 childhood cancer survivors (median follow-up, 23.3 years; range, 5.0–52.2 years), 97 patients developed a benign meningioma, including 80 after full-volume cranial radiation and 14 after partial-volume cranial radiation.
- The 40-year cumulative incidence of meningioma after any cranial radiation was 12.4% (95% CI, 9.8%–15.2%).
- Compared with cranial radiation doses of 1 to 19 Gy, no cranial radiation was associated with a low meningioma risk (HR, 0.04; 95% CI, 0.01–0.15), while increased risks were observed for doses of 20 to 39 Gy (HR, 1.66; 95% CI, 0.83–3.33) and 40 Gy or higher (HR, 2.81; 95% CI, 1.30–6.08).
- Survivors diagnosed before the age of 5 years showed significantly increased risks (HR, 2.38; 95% CI, 1.39–4.07) compared with patients diagnosed between the ages of 10 and 17 years.
- Radiation volume was not significantly associated with increased risk (HR for full vs. partial volume, 1.66; 95% CI, 0.86–3.22) and dose effects did not vary significantly according to exposure age or radiation volume.
- Treatment with carboplatin was associated with meningioma risk (HR, 3.55; 95% CI, 1.62–7.78), but a dose-response was not observed, and all nine exposed cases had received high-dose cranial radiation.
- In a follow-up study from the DCOG-LATER cohort, 90% of survivors with meningioma presented with symptoms rather than through late effects clinic screening, and 32% of survivors presented with synchronous meningiomas.[11]
- CCSS investigators have also evaluated associations between chemotherapy and subsequent malignant neoplasms (SMNs) among nonirradiated, long-term survivors.[12]
- Of 1,498 SMNs in 1,344 survivors, 229 occurred in 206 survivors who were treated with chemotherapy only.
- The 30-year SMN cumulative incidence was 3.9% for the chemotherapy-only group, 9.0% for the chemotherapy-plus-radiation group, 10.8% for the radiation-only group, and 3.4% for the neither-treatment group.
- SIRs for SMNs were increased for any SMN (SIR, 2.8), subsequent leukemia/lymphoma (SIR, 1.9), breast cancer (SIR, 4.6), soft tissue sarcoma (SIR, 3.4), thyroid cancer (SIR, 3.8), and melanoma (SIR, 2.3).
- The SMN rate was significantly associated with exposure to platinum chemotherapy doses higher than 750 mg/m2 (relative rate, 2.7) and alkylating agents (relative rate, 1.2 per 5,000 mg/m2).
- The breast cancer rate showed a linear dose response (relative rate, 1.3 per 100 mg/m2) with anthracycline exposure.
- DCOG-LATER investigators evaluated the contribution of chemotherapy to solid cancer risk in a large cohort of childhood cancer survivors diagnosed between 1963 and 2001 (median follow-up, 20.7 years).[13]
- The 25-year cumulative SN incidence was 3.9% and did not change across decades.
- Survivors treated with doxorubicin exhibited a dose-dependent increased risk of all solid cancers and breast cancer. This relationship was stronger in survivors with Li-Fraumeni syndrome–associated childhood cancers (leukemia, central nervous system [CNS], and sarcomas other than Ewing) than in survivors of other cancers.
- Among female survivors who did not receive chest radiation or total-body irradiation (TBI) and developed breast cancer (n = 31), HRs for doxorubicin dose tertiles were 1.3 (95% CI, 0.3–6.1), 5.6 (95% CI, 1.9–16.2), and 9.9 (95% CI, 4.2–23.8).
- A dose-response relationship was confirmed with cyclophosphamide and subsequent sarcoma, particularly bone sarcoma. The HR for subsequent sarcoma was 3.1 (95% CI, 1.5–6.0) for survivors who received cyclophosphamide at a dose greater than 9,400 mg/m2 and 2.6 (95% CI, 1.3–5.2) for those who received ifosfamide.
- St. Jude Life (SJLIFE) cohort study investigators assessed the contribution of pathogenic and likely pathogenic variants in cancer predisposition genes to SN risk in childhood cancer survivors.[14]
- Of 3,006 study participants evaluated by whole-genome sequencing (30-fold), 1,120 SNs were diagnosed among 439 survivors (14.6%), and 175 pathogenic or likely pathogenic variants were identified in 5.8% of survivors. The prevalence of a pathogenic or likely pathogenic variant among nonirradiated survivors with SNs was much higher, at 18%.
- Variants were associated with significantly increased rates of breast cancer (relative risk [RR], 13.9) and sarcoma (RR, 10.6) among irradiated survivors and with developing any SN (RR, 4.7), breast cancer (RR, 7.7), nonmelanoma skin cancer (RR, 11), and two or more histologically distinct SNs (RR, 18.6).
- Variant carriers did not have an increased rate of meningioma or thyroid cancer.
The incidence and type of SNs depend on the following:
- Primary cancer diagnosis.
- Type of therapy received.
- Presence of genetic conditions.
Unique associations with specific therapeutic exposures have resulted in the classification of SNs into the following two distinct groups:
- Myelodysplastic syndrome postcytotoxic therapy (MDS-pCT) and acute myeloid leukemia postcytotoxic therapy (AML-pCT) (previously termed t-MDS and t-AML).
- Therapy-related solid SNs.
Myelodysplastic Syndrome and Acute Myeloid Leukemia Postcytotoxic Therapy (MDS-pCT and AML-pCT)
Subsequent primary leukemias have been reported in survivors of Hodgkin lymphoma, leukemia, sarcoma, CNS tumors, non-Hodgkin lymphoma, neuroblastoma, and Wilms tumor. In a cohort of nearly 70,000 5-year childhood cancer survivors, survivors had a fourfold increased risk (SIR, 3.7) of developing a leukemia, with an absolute excess risk of 7.5. Specifically, a sixfold relative risk of developing a myeloid leukemia (SIR, 5.8) was reported.[15]
- The risk remained significantly elevated beyond 20 years from the first primary malignancy (SIR, 2.4).
- Hodgkin lymphoma survivors had the greatest excess risk of developing a subsequent leukemia (SIR, 7.9) and specifically a myeloid leukemia (SIR, 12.1), with the largest excess risk seen before 20 years of follow-up.
A pooled analysis examined all published studies with detailed treatment data for children with cancer diagnosed between 1930 and 2000. Treatment data included estimated radiation doses to the active bone marrow and doses of specific chemotherapy agents. In this report, 147 cases of second primary leukemia (69% of cases were AML) were matched to 522 controls.[16]
- After controlling for other therapies, topoisomerase II inhibitor therapy was associated with an increased risk of second AML (no radiation and >2,500 mg/m2 vs. none: OR, 14.3; 95% CI, 2.7–75.1).
- Radiation dose to the active bone marrow was also associated with an increased risk of second AML among patients who did not receive chemotherapy (>0–12 Gy: OR, 4.9; 95% CI, 0.95–25.6) but not among those who received chemotherapy.
- Second primary leukemias were most likely to occur in the first decade after cancer treatment.[17]
Characteristics of MDS-pCT and AML-pCT include the following:[18,19]
- A short latency (<10 years from primary cancer diagnosis). The risk of MDS-pCT or AML-pCT plateaus after 10 to 15 years. Although the risk of subsequent leukemia remains significantly elevated beyond 15 years from primary diagnosis (SIR, 3.5; 95% CI, 1.9–6.0), these events are relatively rare, with an absolute excess risk of 0.02 cases per 1,000 person-years.[19]
- An association with alkylating agents and/or topoisomerase II inhibitors.
Based on the updated definitions from the World Health Organization, MDS-pCT and AML-pCT are clonal disorders, which arise in patients previously exposed to cytotoxic therapy, either chemotherapy or large-field radiation therapy, for an unrelated neoplasm.[20] The following two types of MDS-pCT and AML-pCT are the most frequently observed among survivors:
- Alkylating agent–related type: Alkylating agents associated with MDS-pCT and AML-pCT include cyclophosphamide, ifosfamide, mechlorethamine, melphalan, busulfan, nitrosoureas, chlorambucil, and dacarbazine.[21]
The risk of alkylating agent–related MDS or AML is dose dependent, with a latency of 3 to 5 years after exposure; it is associated with abnormalities involving chromosomes 5 (-5/del(5q)) and 7 (-7/del(7q)).[21]
- Topoisomerase II inhibitor–related type: Topoisomerase II inhibitor agents include etoposide, teniposide, and anthracycline-related drugs.
Most of the translocations observed in patients exposed to topoisomerase II inhibitors disrupt a breakpoint cluster region between exons 5 and 11 of the band 11q23 and fuse KMT2A with a partner gene.[21] Topoisomerase II inhibitor–related AML presents as overt leukemia after a latency of 6 months to 3 years and is associated with balanced translocations involving chromosome bands 11q23 or 21q22.[22]
For more information, see the Therapy-Related AML and Therapy-Related Myelodysplastic Neoplasms section in Childhood Acute Myeloid Leukemia Treatment.
Therapy-Related Solid SNs
Therapy-related solid SNs represent 80% of all SNs, demonstrate a strong relationship with radiation exposure, and are characterized by a latency that exceeds 10 years. The risk of solid SNs continues to increase with longer follow-up. The risk of solid SNs is highest when the following occur:[4,13]
- Younger age at time of radiation exposure.
- High total dose of radiation.
- Longer period of follow-up after radiation exposure.
The histological subtypes of solid SNs encompass a neoplastic spectrum ranging from benign and low-grade malignant lesions (e.g., NMSC, meningiomas) to high-grade malignancies (e.g., breast cancers, glioblastomas) (see Figure 4).[4,13,23,24]
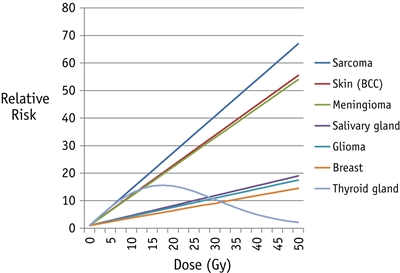
Figure 4. Fitted radiation dose-response by type of second cancer, based on previously published studies of second sarcoma, skin, meningioma, salivary gland, glioma, breast, and thyroid gland. The order of second cancers from top to bottom in the graph is the same as in the key to the right of the panel. Reprinted from International Journal of Radiation Oncology*Biology*Physics, Volume 94, Issue 4, Inskip PD, Sigurdson AJ, Veiga L, et al., Radiation-Related New Primary Solid Cancers in the Childhood Cancer Survivor Study: Comparative Radiation Dose Response and Modification of Treatment Effects, Pages 800–807, Copyright © 2016, with permission from Elsevier.
Solid SNs in childhood cancer survivors most commonly involve the following:[4,13,23,25,26,27,28]
With longer follow-up of adult survivors of childhood cancer cohorts, epithelial neoplasms have been observed in the following:[13,29]
Benign and low-grade SNs, including NMSCs and meningiomas, have also been observed with increasing prevalence in survivors who were treated with radiation therapy for childhood cancer.[4,10,30]
Subsequent neoplasms after hematopoietic stem cell transplant (HSCT)
Recipients of HSCT are treated with high-dose chemotherapy and, often, TBI, which makes their risk of SNs unique from that of the general oncology population.
- Among 4,318 first-time allogeneic HSCT recipients treated for AML and chronic myeloid leukemia between 1986 and 2005, and conditioned with high-dose busulfan and cyclophosphamide (Bu-Cy), 66 solid cancers were reported at a median of 6 years post-HSCT.[31]
- The cumulative incidence of new solid cancers was 0.9% at 5 years and 2.4% at 10 years and appears to be similar, regardless of exposure to radiation.
- Bu-Cy conditioning without TBI was associated with higher risks of solid SNs than in the general population.
- Chronic graft-versus-host disease increased the risk of SNs, especially those involving the oral cavity.
- A study of 4,905 1-year survivors of allogeneic HSCT who underwent transplant between 1969 and 2014 for malignant or nonmalignant diseases, and were followed for a median 12.5 years, demonstrated a strong effect of TBI dose and dose fractionation on risk of SNs.[32]
- The 20-year cumulative incidence of SN after HSCT for individuals treated at younger than 20 years was 8.1%.
- SN risk was highest in survivors exposed to high-dose, single-fraction TBI (6–12 Gy) or very high-dose fractionated TBI (14.4–17.5 Gy).
- With low-dose TBI (2–4.5 Gy), the SN risk was comparable to the risk with chemotherapy alone, although it was still twofold higher than in the general population.
- Among individuals treated at younger than 20 years, the number of SNs was 12.5-fold higher than expected in the general population, and the excess absolute risk was 10.6 per 1,000 person-years. Survivors treated with HSCT at this young age were more likely to develop SNs than were survivors who were treated after age 50 years (HR, 2.3).
Some well-established solid SNs are described in the following sections.
Breast cancer
Female survivors of childhood, adolescent, and young adult cancer treated with radiation therapy to fields including the chest are at increased risk of developing breast cancer.
- The cumulative breast cancer incidence ranges from 8% to 20% by age 40 to 45 years among childhood cancer survivors and is as high as 35% by age 50 years in Hodgkin lymphoma survivors, comparable to that observed among BRCA gene variant carriers.[18,33,34,35,36]
- Radiation dose and volume of breast exposed are important factors affecting risk. Specific chemotherapeutic agents, particularly alkylating agents and anthracyclines, may affect risk as well.[33,35,37]
Evidence (excess risk of breast cancer):
- Breast cancer is the most common therapy-related solid SN after a previous diagnosis of Hodgkin lymphoma.[18,34] The following has been observed in female survivors of childhood Hodgkin lymphoma:
- Excess risk of breast cancer has been reported in survivors treated with high-dose, extended-volume radiation at age 30 years or younger.[38]
- Data indicate that females treated with low-dose, involved-field radiation also exhibit excess breast cancer risk.[39]
- Patients who received limited volume supradiaphragmatic radiation therapy (excluding the axillae) had a significantly lower risk of subsequent breast cancers than patients who received full mantle-field radiation therapy.[37]
- For patients treated with radiation therapy to the chest before age 16 years, the cumulative incidence of breast cancer approaches 20% by age 45 years.[18]
- The latency period after chest irradiation ranges from 8 to 10 years, and the risk of subsequent breast cancer increases in a linear fashion with radiation dose (P for trend < .001).[40]
- Treatment with higher cumulative doses of alkylating agents and ovarian radiation of 5 Gy or higher (exposures predisposing to premature menopause) have been correlated with reductions in breast cancer risk, underscoring the potential contribution of hormonal stimulation on breast carcinogenesis.[37,41,42]
- The observed number of invasive breast cancer cases among young (aged <30 years) survivors, compared with what is expected in the general population, has decreased over recent treatment eras (1970s SIR, 55.0 vs. 1990s SIR, 14.3).[36]
- The risk of breast cancer was also increased in the following studies that used lower radiation doses to treat cancer that metastasized to the chest/lung (e.g., Wilms tumor, sarcoma) and exposed the breast tissue:
- In 116 children in the CCSS cohort treated with 2 Gy to 20 Gy to the lungs (median, 14 Gy), the SIR for breast cancer was 43.6 (95% CI, 27.1–70.1).[35]
- A report of 2,492 female participants in the National Wilms Tumor Studies 1 through 4 (1969–1995) addressed the excess risk of breast cancer.[43]
- Sixteen of 369 women who received chest irradiation for metastatic Wilms tumor developed invasive breast cancer (cumulative risk at age 40 years, 14.8% [95% CI, 8.7%–24.5%]). The SIR of 27.6 (95% CI, 16.1–44.2) was based on 5,010 person-years of follow-up.
- Of the 369 patients, radiation doses to the chest were less than 12 Gy in 4%, 12 Gy in 64%, 13 Gy to 15 Gy in 19%, and more than 15 Gy in 13% of patients.
- For all patients who developed breast cancer (with or without chest irradiation), the median age at first breast cancer diagnosis was 34.3 years (range, 15.5–48.4) and the median time from Wilms tumor diagnosis was 27.1 years (range, 7.9–35.7).
- An international collaborative study pooled individual patient data from 17,903 childhood cancer survivors. The study evaluated the dose-dependent effects of individual anthracycline agents on the development of subsequent breast cancer and interactions with chest radiation therapy. There were 782 survivors (4.4%) who developed a subsequent breast cancer.[44]
- Doxorubicin was associated with a dose-dependent increase of subsequent breast cancer risk (HR per 100 mg/m2, 1.24; 95% CI, 1.18–1.31).
- There was a more-than-twofold increased risk for survivors treated with 200 mg/m2 or higher cumulative doxorubicin dose, compared with no doxorubicin (HR, 2.50 for 200–299 mg/m2; HR, 2.33 for 300–399 mg/m2; HR, 2.78 for ≥400 mg/m2).
- The associations were not statistically significant for daunorubicin, whereas epirubicin was associated with increased subsequent breast cancer risk (exposure yes vs. no: HR, 3.25; 95% CI, 1.59–6.63).
- The HRs per 100 mg/m2 of doxorubicin were 1.11 (95% CI, 1.02–1.21) for patients treated with chest radiation therapy and 1.26 (95% CI, 1.17–1.36) for patients who did not receive chest radiation therapy.
- The risk of developing breast cancer after radiation therapy and chemotherapy with anthracyclines was evaluated in the CCSS. In a nested-case control study of 271 childhood cancer survivors (diagnosed between 1970–1986) who were subsequently diagnosed with breast cancer, the combination of anthracyclines and radiation therapy to the breast was associated with increased risks of breast cancer consistent with an additive interaction.[33]
- For the study group, the median age of first cancer diagnosis was 15 years and the median age at breast cancer diagnosis was 39 years.
- The OR for breast cancer increased with increasing radiation dose to the breast (OR per 10 Gy, 3.9; 95% CI, 2.5–6.5) and was similar for estrogen receptor–positive and estrogen receptor–negative cancers.
- The OR per 10 Gy to the breast was higher for women who received ovarian doses less than 1 Gy (OR, 6.8; 95% CI, 3.9–12.5) than for women who received ovarian doses greater than or equal to 15 Gy (OR, 1.4; 95% CI, 1.0–6.4).
- The OR for breast cancer increased with cumulative anthracycline dose (OR per 100 mg/m2, 1.23; 95% CI, 1.09–1.39; P < .01 for trend).
- There was an additive interaction between radiation therapy and anthracycline treatment. The OR was 19.1 (95% CI, 7.6–48.0) for the combined association of anthracycline therapy and breast radiation dose of 10 Gy or more (compared with 0 to less than 1 Gy) versus 9.6 (95% CI, 4.4–20.7) without anthracycline therapy.
- Childhood cancer survivors not exposed to chest radiation also have an increased risk of breast cancer at a young age.
- The SJLIFE study assessed subsequent breast cancer risk among 1,467 female cancer survivors and evaluated risk associated with anthracycline exposure. The study also evaluated whether surveillance imaging affects breast cancer outcomes.[25]
- In women who received neither chest radiation nor anthracyclines, the cumulative incidence of breast cancer was 2% at age 35 years and 15% at age 50 years. For women who were treated with 250 mg/m2 or higher of anthracyclines, the rates were 7% at age 35 years and 46% at age 50 years.
- Anthracycline doses of 250 mg/m2 or higher remained significantly associated with increased risk of breast cancer in models, excluding survivors with cancer predisposition gene variants, chest radiation of 10 Gy or higher, or both.
- Breast cancers detected by imaging and/or prophylactic mastectomy were more likely to be in situ carcinomas, be smaller masses, have no lymph node involvement, and be treated without chemotherapy, compared with breast cancers detected by physical findings.
- Dual imaging with mammography and breast magnetic resonance imaging (MRI) in this cohort was a sensitive and specific approach to identify breast cancers that require less aggressive therapy than breast cancers detected by physical findings.
- A CCSS investigation examined the breast cancer risk of 3,768 female participants who did not receive chest radiation.[45]
- A fourfold excess risk (SIR, 4.0; 95% CI, 3.0–5.3) of breast cancer was observed compared with rates in the general population.
- Breast cancer risk was highest among survivors of sarcoma (SIR, 5.3; 95% CI, 3.6–7.8) and leukemia (SIR, 4.1; 95% CI, 2.4–6.9), for whom the cumulative incidence of breast cancer was estimated to be 5.8% and 6.3%, respectively, by age 45 years.
- Treatment with alkylating agents and anthracyclines increased the risk of breast cancer in a dose-dependent manner.
- CCSS investigators also examined SN risk among 7,448 participants who were treated with chemotherapy only.[12]
- Breast cancer incidence was 4.6-fold greater than what would be expected in the general population (SIR, 4.6; 95% CI, 3.5–6.0).
- A linear dose response was demonstrated between anthracyclines and breast cancer rate (RR, 1.3/100 mg/m2; 95% CI, 1.2–1.6).
- DCOG-LATER investigators evaluated the contribution of chemotherapy to solid cancer risk in a large cohort of childhood cancer survivors diagnosed between 1963 and 2001.[13]
- Survivors treated with doxorubicin exhibited a dose-dependent increased risk of breast cancer (HR, 3.1; 95% CI, 1.4–6.5 among survivors treated with anthracycline doses of 250 mg/m2 or higher).
- The doxorubicin–breast cancer dose response was stronger for survivors of Li-Fraumeni–associated cancers (leukemia, CNS, and sarcomas other than Ewing) than for survivors of other cancers.
- The SJLIFE study assessed subsequent breast cancer risk among 1,467 female cancer survivors and evaluated risk associated with anthracycline exposure. The study also evaluated whether surveillance imaging affects breast cancer outcomes.[25]
- A SEER Program–based study evaluated trends in surgical management and the 5- and 10-year cumulative incidence of contralateral breast cancer among women who were treated with radiation therapy for Hodgkin lymphoma before age 30 years and diagnosed with a subsequent breast cancer between 1990 and 2016.[46]
- Overall, 263 (89.2%) women presented with unilateral breast cancer, 50 of whom (19.0%) underwent breast-conserving surgery and 213 of whom (81.0%) underwent mastectomy (40.5% bilateral).
- The 5-year incidence of contralateral breast cancer in women who underwent unilateral surgery was 9.4% (95% CI, 5.6%–15.4%), increasing to 20.2% (95% CI, 13.7%–29.2%) at 10 years and 29.9% (95% CI, 20.8%–41.9%) at 15 years. This finding underscores the importance of ongoing breast cancer surveillance and consideration of prophylactic mastectomy.
Breast cancer risk varies among childhood cancer survivors who are treated with chest radiation therapy, and the risk is based on multiple clinical factors. The first personalized breast cancer risk prediction model was developed and validated using multinational cohorts of female 5-year cancer survivors who were diagnosed at younger than 21 years and treated with chest irradiation (n = 2,147). The model includes current age, chest radiation field, whether chest radiation was delivered within 1 year of menarche, anthracycline exposure, age of menopause, and history of a first-degree relative with breast cancer. The model is available as an online risk calculator.[47]
Subsequent versus de novo breast cancer
Several studies have investigated the clinical characteristics of subsequent breast cancers arising in women treated with radiation therapy for childhood cancer.[48,49,50,51,52]
- In one population-based study, radiation-induced breast cancer was noted to have more adverse clinicopathological features, as evidenced by a twofold increased risk of estrogen receptor–negative, progesterone receptor–negative breast cancer observed among 15-year Hodgkin lymphoma survivors, compared with women who had sporadic breast cancer.[48]
- Other studies have observed a higher proportion of more histologically aggressive subtypes (e.g., triple-negative breast cancer) than age-matched sporadic invasive cancers.[49,50]
- These findings are in contrast to other smaller, hospital-based, case-control studies of breast cancer among Hodgkin lymphoma survivors that have not identified a significant variation in hormone receptor status when compared with primary breast cancer controls. Previous studies have also not demonstrated a significant difference in overall risk of high-grade versus low-grade tumors.[51,52]
- A study using SEER Program data evaluated the clinicopathological features of 321 breast cancers diagnosed in 257 women (median age, 22 years; range, 18–26 years at Hodgkin lymphoma diagnosis) who were previously treated with radiation for Hodgkin lymphoma.[53]
- Women who developed breast cancer after radiation for Hodgkin lymphoma were younger than women diagnosed with breast cancer without a prior malignancy (43 vs. 60 years) and were less likely to present with ductal carcinoma in situ (0.4% vs. 14.9%).
- Radiation was not associated with poorer biological features, compared with breast cancers diagnosed in similarly aged women with no prior malignancy. However, higher proportions of upper outer quadrant and smaller tumors (≤2 cm) were found.
- Most tumors in survivors of Hodgkin lymphoma were hormone sensitive (nearly two-thirds were estrogen receptor–positive/HER2-negative). This finding suggests that endocrine prevention may be an option for this high-risk population.
Mortality after subsequent breast cancer
In a study of female participants in the CCSS who were subsequently diagnosed with breast cancer (n = 274) and matched to a control group of women (n = 1,095) with de novo breast cancer, the following was observed:[54]
- Survivors of childhood cancer were found to have elevated mortality rates (HR, 2.2; 95% CI, 1.7–3.0), even after adjusting for breast cancer treatment.
- Survivors were five times more likely to die from other health-related causes, including other SMNs and cardiovascular or pulmonary disease (HR, 5.5; 95% CI, 3.4–9.0).
- The cumulative incidence of a second asynchronous breast cancer was elevated significantly compared with controls (at 5 years, 8.0% among childhood cancer survivors vs. 2.7% among controls; P < .001).
Although current evidence does not show a survival benefit from the initiation of breast cancer surveillance in women treated with radiation therapy to the chest for childhood cancer, interventions to promote detection of small and early-stage tumors may improve prognosis. Those with more limited treatment options because of previous exposure to radiation or anthracyclines may especially benefit.
In support of surveillance, SJLIFE investigators observed that breast cancers detected by imaging and/or prophylactic mastectomy were more likely to be in situ carcinomas, be smaller masses (3.3 cm mean tumor size detected by physical examination vs. 1.1 cm detected by imaging), have no lymph node involvement, and be treated without chemotherapy, compared with breast cancers detected by physical findings.[25]
Investigators used data from the CCSS and two Cancer Intervention and Surveillance Modeling Network breast cancer simulation models to estimate the clinical benefits, harms, and cost-effectiveness of breast cancer screening among childhood cancer survivors who were previously treated with chest radiation.[55]
- Screening with mammography and MRI, as recommended in COG Long-Term Follow-Up guidelines, is projected to avert half of the expected breast cancer deaths among high-risk survivors.
- On an annual schedule, a survivor will have an average of 4 to 5 false-positive screening results and 1 to 2 benign biopsy results over the course of their lifetime.
- Because of the large survival benefits, the harm-benefit tradeoffs for survivors were found to be appropriate, resulting in more favorable harm-benefit ratios.
Another CCSS investigation quantified the association between temporal changes in cancer treatment over three decades and subsequent breast cancer risk.[36]
- The cumulative incidence of breast cancer was 8.1% (95% CI, 7.3%–9.0%) by age 45 years among 11,550 female survivors (median age, 34.2 years), representing a more than sixfold excess risk (SIR, 6.6; 95% CI, 6.1–7.2), compared with age-, sex-, and calendar year–matched controls.
- Concurrent with changes in therapy by decade, including reduced rates of chest and pelvic radiation therapy and increased rates of anthracycline chemotherapy exposure, and adjusting for age and age at diagnosis, the invasive breast cancer rate decreased 18% for every 5 years of primary cancer diagnosis era (rate ratio, 0.82; 95% CI, 0.74–0.90). This finding was largely associated with the reduced rate of chest radiation therapy.
Thyroid cancer
Thyroid cancer is observed after the following:[12,24,56,57]
- Neck radiation therapy for Hodgkin lymphoma, acute lymphoblastic leukemia (ALL), and brain tumors.
- Iodine I 131-metaiodobenzylguanidine (131I-MIBG) treatment for neuroblastoma.
- TBI for HSCT.
- Chemotherapy only, without therapeutic radiation.
The 25-year cumulative incidence of thyroid cancer among survivors of childhood cancer is 0.5%.[13] The risk of thyroid cancer among childhood cancer survivors is more than tenfold higher than that of the general population (SIR, 10.5; 95% CI, 9.1–12).[4] Significant modifiers of the radiation-related risk of thyroid cancer include the following:[28,58]
- Female sex.
- Younger age at exposure.
- Longer time since exposure.
- Radiation dose. A linear dose-response relationship between radiation exposure and thyroid cancer is observed up to 10 Gy, with a leveling off between 10 Gy and 30 Gy, and a decline in the OR at higher doses, especially in children younger than 10 years at treatment, suggesting a cell killing effect of the target cells at higher doses.[24,28,59]
In a Dutch case-control study, childhood cancer survivors with subsequent thyroid cancer were more likely to present with smaller tumors and bilateral tumors than the general population. Treatment outcomes were similar between subsequent and sporadic thyroid cancers.[60]
For information about detecting thyroid nodules and thyroid cancer, see the Thyroid nodules section.
CNS tumors
Subsequent CNS tumors represent a spectrum of histological subtypes, from high-grade gliomas to benign meningiomas. A comprehensive Pediatric Normal Tissue Effects in the Clinic (PENTEC) review analyzed the risk of SNs. The study reported a 10-year median latency period for the development of a malignant CNS neoplasm and a 21-year median latency period for the development of a meningioma.[61] Accurate assessment of the prevalence of low-grade and benign lesions is challenging because of the variable opinions and practices related to neuroimaging versus symptom surveillance in long-term survivors treated with cranial irradiation. Therefore, the prevalence of these tumors is likely higher than proven.
Brain tumors develop after cranial irradiation for histologically distinct brain tumors or for management of disease among ALL or non-Hodgkin lymphoma patients.[62] SIRs reported for subsequent CNS neoplasms after treatment for childhood cancer range from 8.1 to 52.3 across studies.[24]
The risk of subsequent brain tumors demonstrates a linear relationship with radiation dose.[26,61,63]
- The risk of meningioma after radiation increases with radiation dose,[9,61] and in some studies is further potentiated with increased exposure to intrathecal methotrexate.[26] However, this finding has not been consistently replicated.[10]
- Cavernomas have also been reported with considerable frequency after CNS irradiation but have been speculated to result from angiogenic processes as opposed to true tumorigenesis.[64,65,66]
The Dutch Long-Term Effects after Childhood Cancer (LATER) investigators have described the clinical characteristics of childhood cancer survivors who developed histologically confirmed meningiomas.[11]
- In 6,015 childhood cancer survivors from the LATER cohort, 1,551 of whom had prior cranial radiation therapy, 93 survivors developed meningiomas.
- Of these patients, 89 (95.7%) were treated with prior cranial radiation therapy. The median age at diagnosis was 31.8 years (range, 13.2–50.5 years).
- Thirty of the survivors presented with synchronous meningiomas, and 84 survivors presented with symptoms. Only 16% of the meningiomas were detected in late effects clinics.
- All survivors underwent surgery, and one-third (n = 31) of them also received radiation therapy. Twelve survivors had three or more surgeries for growth of residual tumor, recurrences, and new meningiomas. Although the extent of surgical resection was not described, the indications for radiation therapy during follow-up after surgical resection included residual tumor, recurrences, location, or new meningioma. During follow-up, 38 survivors (40.9%) developed new meningiomas, 22 (23.7%) had recurrences, and at least 4 died because of the meningioma.
The European PanCare Childhood and Adolescent Cancer Survivor Care and Follow-Up Studies (PanCareSurFup) investigators described findings in childhood cancer survivors who developed meningiomas or gliomas:[67]
- In 69,460 survivors, 279 developed gliomas, and 761 developed meningiomas.
- Gliomas and meningiomas were most frequently observed after any CNS tumor or leukemia, accounting for more than 70% of all observed gliomas and 80% of all meningiomas.
- Among patients with known cranial radiation status who developed a glioma, 61% had received prior cranial radiation therapy. Among patients who developed a meningioma, 64.7% had received cranial radiation therapy.
- CNS tumor survivors treated with cranial radiation therapy were at the highest risk of developing gliomas, at 27 times the risk of the general population (95% CI, 21.5–33.2). CNS tumor survivors who did not receive cranial radiation were at 8.3 times the risk of the general population (95% CI, 4.9–14.1).
- Among CNS tumor survivors, the relative risk for patients who received cranial radiation therapy was 13 times the risk for patients who did not receive cranial radiation therapy (95% CI, 6.7–25.4). Among leukemia survivors, those who received cranial radiation therapy were at a 5-fold increased risk compared with those treated without cranial radiation therapy (95% CI, 2.9–9.9).
A PENTEC analysis of CNS SNs included 32 published studies of 1,035 subsequent meningiomas after previous radiation therapy in childhood cancer survivors.[61]
- A significant dose-response relationship was reported for CNS subsequent meningiomas (excess relative ratio [ERR]/Gy, 0.44).
- Younger age at the time of primary diagnosis was associated with a higher risk of subsequent meningiomas.
- Females had a higher risk of subsequent meningiomas than males (odds ratio, 1.46; P < .0001).
- Median latency time to the development of meningiomas was 21 years.
Neurological sequelae associated with meningiomas can include seizures, auditory-vestibular-visual deficits, focal neurological dysfunction, and severe headaches.[9] Despite the well-established increased risk of subsequent CNS neoplasms among childhood cancer survivors treated with cranial irradiation and the growing recognition of associated morbidity, the current literature is insufficient to evaluate the potential harms and benefits of routine screening for these lesions.[68] The decision to initiate surveillance should be shared by the cancer survivor and health care provider after carefully considering the potential harms and benefits of surveillance for CNS neoplasms, such as meningioma.
Proton radiation therapy for pediatric medulloblastoma is associated with low rates of brain stem injury and secondary malignancies. The long-term effects were reported in 178 pediatric patients with medulloblastoma who were treated with surgery, proton radiation therapy, and chemotherapy between 2002 and 2016 (median follow-up, 9.3 years).[69]
- At 10 years, eight patients (4.5%) developed a secondary tumor (benign or malignant), with median follow up of 9.1 years. Three patients (1.7%) developed a secondary malignancy.
- In-field second malignancies were glioblastoma (n = 2), meningioma (n = 2), and high-grade glioma (n = 1). The other malignancies were one each of ovarian fibroma, plexiform fibromyxoma of the esophagus, and papillary thyroid carcinoma.
- Four patients developed brain stem injury at a median of 4.2 years. The 5-year cumulative incidence of brain stem injury was 1.1%, and the 10-year cumulative incidence was 1.9%.
Bone and soft tissue tumors
Survivors of hereditary retinoblastoma, Ewing sarcoma, and other malignant bone tumors are at a particularly increased risk of developing subsequent bone and soft tissue tumors.[70,71,72,73,74]
- Radiation therapy is associated with a linear dose-response relationship.[75,76]
- In a PENTEC investigation on subsequent malignancies, the estimated pooled ERR/Gy for subsequent sarcomas was 0.045. There was a possible biphasic dose response, with higher rates of relapse and subsequent sarcomas above 55 Gy. After 20 Gy and anthracyclines, the absolute excess risk is predicted to be 0.24% at 50 years and 0.86% at 75 years. The median latency time to the development of sarcomas was 11 years (range, 4–23 years).[61]
- After adjustment for radiation therapy, treatment with alkylating agents [13,61] and anthracyclines [77] have both been linked to sarcoma, with the risk increasing with cumulative drug exposure.[77]
- Soft tissue sarcomas can be of various histological subtypes, including nonrhabdomyosarcoma soft tissue sarcomas, rhabdomyosarcoma, malignant peripheral nerve sheath tumors, Ewing/primitive neuroectodermal tumors, and other rare tumor types.
Evidence (excess risk of bone and soft tissue tumors):
- A nested case-control study included 228 cases and 228 matched controls within a cohort of 69,460 5-year survivors of childhood cancer. The study investigated the risks of subsequent primary bone cancer by different levels of cumulative radiation exposure and dose-response relationships according to different specific types of chemotherapy.[78]
- Compared with unexposed bone tissue, the OR associated with bone tissue exposed to 1 to 4 Gy was 4.8-fold (95% CI, 1.2–19.6). The OR associated with bone tissue exposed to 5 to 9 Gy was 9.6-fold (95% CI, 2.4–37.4). The OR increased linearly with increasing doses of radiation (Ptrend < .001), up to 78-fold (95% CI, 9.2–669.9) for doses of 40 Gy or higher.
- For cumulative alkylating agent doses of 10,000 to 19,999 mg/m2 and 20,000 mg/m2 or higher, the radiation-adjusted ORs were 7.1 (95% CI, 2.2–22.8) and 8.3 (95% CI, 2.8–24.4), respectively. There were independent contributions from exposure to procarbazine, ifosfamide, or cyclophosphamide.
- A population-based study of 69,460 5-year survivors of cancer diagnosed before age 20 years observed the following:[71,72]
- The risk of subsequent primary bone cancer was 22-fold greater than that of the general population, with an estimated 45-year cumulative incidence of 0.6%, compared with an expected rate of 0.03% in the general population.[71]
- The observed excess numbers of subsequent primary bone cancer declined with both age and years from diagnosis.[71]
- The risk of subsequent soft tissue sarcoma was almost 16-fold higher than the general population, with an estimated 45-year cumulative incidence of 1.4%, compared with an expected rate of 0.1%.[72]
- The median time from diagnosis to occurrence of a soft tissue sarcoma was 19 years.[72]
- The most commonly observed soft tissue sarcomas were leiomyosarcoma, fibromatous neoplasms, and malignant peripheral nerve sheath tumors.[72]
- The SIR for subsequent fibromatous primary sarcomas decreased with increasing years from diagnosis and attained age, whereas the SIR for leiomyosarcoma and malignant peripheral nerve sheath tumors remained consistently high across all years from diagnosis and at all attained ages.[72]
- The absolute excess risks of all sarcoma subtypes were generally low, except for leiomyosarcoma that followed a retinoblastoma diagnosis (absolute excess risks, 52.7 per 10,000 person-years among survivors 45 years or more from diagnosis).[72]
- The risk of developing a leiomyosarcoma was 30-fold higher among survivors of childhood cancer, compared with an excess risk of 0.7 for the general population.[72]
- Retinoblastoma survivors were at the highest risk (SIR, 342.9), followed by Wilms tumor survivors (SIR, 74.2).
- 90% of leiomyosarcomas observed after a Wilms tumor diagnosis developed within the irradiated tissue.
- In a CCSS cohort, an increased risk of subsequent bone or soft tissue sarcoma was associated with radiation therapy, a primary diagnosis of sarcoma, a history of other SNs, and treatment with higher doses of anthracyclines or alkylating agents.[27]
- The 30-year cumulative incidence of subsequent sarcoma in CCSS participants was 1.08% for survivors who received radiation therapy and 0.5% for survivors who did not receive radiation therapy.
- Dose-risk modeling was used to study the risk of bone sarcoma in a retrospective cohort of 4,171 survivors of a childhood solid cancer treated between 1942 and 1986 (median follow-up, 26 years).[75]
- Results demonstrated that the risk of bone sarcoma increased slightly up to a cumulative organ-absorbed radiation dose of 15 Gy (HR, 8.2; 95% CI, 1.6–42.9) and then rapidly increased for higher radiation doses (HR for 30 Gy or more, 117.9; 95% CI, 36.5–380.6), compared with patients not treated with radiation therapy.
- The excess RR per Gy in this model was 1.77 (95% CI, 0.62–5.94).
- In survivors of bilateral retinoblastoma, the most commonly observed malignant SN is sarcoma, specifically osteosarcoma.[79,80,81] The contribution of chemotherapy to solid malignancy carcinogenesis was highlighted in a long-term follow-up study of 906 5-year hereditary retinoblastoma survivors who were diagnosed between 1914 and 1996 and observed through 2009.[70]
- Treatment with alkylating agents significantly increased risk of subsequent bone tumors (HR, 1.60; 95% CI, 1.03–2.49) and leiomyosarcoma (HR, 2.67; 95% CI, 1.22–5.85) among members of the cohort.
- Leiomyosarcoma occurrence was more common after treatment with alkylating agent chemotherapy and radiation therapy compared with radiation therapy alone (5.8% vs. 1.6% at age 40 years; P = .01).
- The CCSS reported the following on 105 cases and 422 matched controls in a nested case-control study of 14,372 childhood cancer survivors:[77]
- Soft tissue sarcomas occurred at a median of 11.8 years (range, 5.3–31.3 years) from original diagnoses.
- Any exposure to radiation was associated with increased risk of soft tissue sarcoma (OR, 4.1; 95% CI, 1.8–9.5), which demonstrated a linear dose-response relationship.
- Anthracycline exposure was associated with soft tissue sarcoma risk (OR, 3.5; 95% CI, 1.6–7.7), independent of radiation dose.
- In a cohort of 952 irradiated survivors of hereditary retinoblastoma diagnosed between 1914 and 2006, CCSS investigators observed that elevated bone and soft tissue sarcoma risks differed by age, location, and sex.[81]
- Head and neck bone and soft tissue sarcomas were diagnosed beginning in early childhood and continued well into adulthood (60-year cumulative incidence of 6.8% and 9.3%, respectively).
- Body and extremity bone sarcoma incidence flattened after adolescence (60-year cumulative incidence, 3.5%).
- Body and extremity soft tissue sarcoma incidence was rare until age 30 years, when incidence rose steeply (60-year cumulative incidence, 6.6%) particularly for females (60-year cumulative incidence, 9.4%).
- In a retrospective study of 160 patients with hereditary retinoblastoma who received radiation therapy, no correlation was identified between age (before or after 12 months) at which external-beam radiation therapy was given and development of subsequent malignancy.[73]
- Patients with and without subsequent malignancies did not differ by RB1 variant type. Also, there was no association with variant type and location of SMN, or SMN type and age at diagnosis.
- The study showed that patients who have a low penetrance variant and receive external-beam radiation therapy remain at risk of SMNs and should be cautiously monitored.
Skin cancer
Keratinocyte carcinomas (KCs) (i.e., basal cell carcinomas [BCCs] and squamous cell carcinomas [SCCs], also called nonmelanoma skin cancers [NMSCs]) are one of the most common SNs among childhood cancer survivors and show a strong association with radiation therapy.[4,82,83] Adherence to sun protection behaviors can reduce exposure to UV radiation that may exacerbate risk.
The CCSS performed a randomized, controlled, comparative effectiveness trial to test methods to improve early detection of skin cancer among survivors of childhood cancer at high risk after radiation therapy exposure. Participants were randomly assigned to the experimental arm, which included print materials in combination with mHealth strategies (text messages and use of the Advancing Survivors' Knowledge website), or the control arm. Screening rates improved by 1.5-fold in the experimental arm. Rates of physician skin examination increased from baseline to 12 months, and rates of self-examination increased from baseline to 18 months in all three intervention groups. However, the increase in rates did not differ between the intervention groups.[84]
Evidence (excess risk of KCs):
- An updated analysis of the CCSS confirmed an increased risk of KCs in participants with histories of radiation therapy. Compared with participants who did not receive radiation therapy, CCSS participants treated with radiation therapy had a 4.5-fold increased risk of KCs (95% CI, 3.5–5.9).[83]
- The risk of KCs increased with higher radiation therapy doses. Per 10 Gy of radiation therapy at the KC site, the RR was similar for head/neck (1.0; 95% CI, 1.0–1.1) and extremity sites (1.0; 95% CI, 0.7–1.3). The RR was slightly higher for trunk sites (1.1; 95% CI, 1.0–1.3).
- Allogeneic and autologous HSCT were associated with an increased risk of KCs (RR for allogeneic HSCT, 3.4; 95% CI, 2.4–4.8 and RR for autologous HSCT, 2.3; 95% CI, 1.2–4.2).
- In 5,843 childhood cancer survivors in the DCOG-LATER cohort, investigators found that childhood cancer survivors had a 30-fold increased risk of developing BCCs.[30]
- After a first BCC diagnosis, 46.7% of patients developed additional BCCs.
- BCC risk was associated with any radiation therapy to the relevant radiation field (site of BCC) (HR, 14.32) and with estimated percentage of exposed skin surface area (26%–75%: HR, 1.99; 76%–100%: HR, 2.16 vs. 1%–25% exposed; Ptrend among exposed = .002).
- BCC risk was not associated with prescribed radiation dose and likelihood of sun-exposed skin area.
- Of all chemotherapy groups examined, only vinca alkaloids increased the BCC risk (HR, 1.54).
- The occurrence of a KC as the first SN has been reported to identify a population at high risk of a future invasive malignant SN.[7]
- CCSS investigators observed a cumulative incidence of a malignant neoplasm of 20.3% (95% CI, 13.0%–27.6%) at 15 years among radiation-exposed survivors who developed a KC as a first SN, compared with 10.7% (95% CI, 7.2%–14.2%) among survivors whose first SN was an invasive malignancy.
Malignant melanoma has also been reported as an SN in childhood cancer survivor cohorts, although at a much lower incidence than NMSCs.
Risk factors for malignant melanoma identified among these studies include the following:[85]
- Radiation therapy (>40 Gy).
- Alkylating agents.
- Bleomycin.
Evidence (excess risk of melanoma):
- Investigators assessed the incidence, risk factors, and outcomes for patients with melanoma in the CCSS cohort (n = 25,716).[85]
- There were 160 survivors (median attained age, 33 years) who developed 177 melanomas (110 invasive, 62 in situ cutaneous, 5 ocular).
- The 40-year cumulative incidence was 1.1% for all participants and 1.5% for those who received cumulative radiation doses of 40 Gy or higher. The standard incidence ratios were 2.0 when compared with the general population.
- An increase in cutaneous melanomas was associated with a cumulative radiation dose of 40 Gy or higher to the site of the melanoma (HR, 2.0), cumulative cyclophosphamide equivalent dose of 20,000 mg/m2 or higher (HR, 1.9), and bleomycin exposure (HR, 2.2).
- The presence of an invasive melanoma was associated with a twofold risk of death.
- A systematic review that included data from 19 original studies (total N = 151,575 survivors; median follow-up of 13 years) observed an incidence of 10.8 cases of malignant melanoma per 100,000 childhood cancer survivors per year.[86]
- Melanomas most frequently developed in survivors of Hodgkin lymphoma, hereditary retinoblastoma, soft tissue sarcoma, and gonadal tumors. However, the relatively small number of survivors represented in the relevant studies preclude assessment of melanoma risk among other types of childhood cancer.
Skin cancer risk after retinoblastoma
The incidence of melanoma and NMSC was evaluated in a cohort of 1,851 long-term, White survivors of retinoblastoma (1,020 hereditary and 831 nonhereditary) who were diagnosed from 1914 to 2006 and monitored through 2016.[87]
- Of all patients, 33 hereditary and 7 nonhereditary survivors developed melanoma, and 26 hereditary and 9 nonhereditary survivors developed NMSC. The median age of skin cancer development was about 20 years younger for hereditary survivors than nonhereditary survivors.
- Most NMSCs were on the head/neck, whereas melanomas were more broadly distributed, with patterns similar to melanoma-prone families.
- At 50 years after retinoblastoma diagnosis, in hereditary survivors, the cumulative incidence of melanoma was 4.5% and the cumulative incidence of NMSC was 3.7%. In nonhereditary survivors, the cumulative incidence of melanoma was 0.7% and the cumulative incidence of NMSC was 1.5%.
Lung cancer
Among childhood cancer survivor cohorts, lung cancer represents a relatively uncommon SN. A PENTEC systematic review reported a median latency period of 25 years (range, 19–29 years) between the childhood cancer diagnosis and the development of a lung SN.[61] The ERR/Gy was 0.068, compared with background cumulative risks. After 20 Gy, the excess absolute risk was predicted to be 0.27% at 50 years. After 50 Gy, the excess absolute risk was predicted to be 0.7% at 50 years.[61]
Evidence (excess risk of lung cancer):
- The 30-year cumulative incidence of lung cancer among CCSS participants was 0.16% (95% CI, 0.09%–0.23%), representing a SIR of 4.0 (95% CI, 2.9–5.4).[88]
- Lung cancer risk demonstrated a dose-related association with chest radiation dose: 10 to 30 Gy (HR, 3.4; 95% CI, 1.05–11.0), more than 30 to 40 Gy (HR, 4.6; 95% CI, 1.5–14.3), and more than 40 Gy (HR, 9.1; 95% CI, 3.1–27.0).
- Cumulative incidence of lung SMNs was higher among current or past smokers, compared with those who had never smoked.
- The SIR for lung cancer was highest among survivors of Hodgkin lymphoma (SIR, 9.3; 95% CI, 6.2–13.4) and bone cancer (SIR, 4.4; 95% CI, 1.8–9.1).
- The 25-year cumulative incidence of lung cancer among the DCOG-LATER cohort was 0.1% (95% CI, 0.0%–0.3%).[13]
- Incidence was approximately fourfold higher than what would be expected in the general population (SIR, 4.3; 95% CI, 1.9–8.5).
- Lung cancer has been reported after chest irradiation for Hodgkin lymphoma.[89]
- The risk increases in association with longer elapsed time from diagnosis.
- Smoking has been linked with the occurrence of lung cancer that develops after radiation therapy for Hodgkin lymphoma.[89]
- The increase in risk of lung cancer with increasing radiation dose is greater among patients who smoke after exposure to radiation than among those who refrain from smoking (P = .04).
Gastrointestinal (GI) cancer
There is substantial evidence that childhood cancer survivors develop GI malignancies more frequently and at a younger age than the general population. This evidence supports the need for early initiation of colorectal carcinoma surveillance.[90,91,92]
Evidence (excess risk of GI cancer):
- In a French and British cohort-nested, case-control study of childhood solid tumor survivors diagnosed before age 17 years, the risk of developing a digestive organ SN varied with therapy.[93]
- The risk of GI cancer was 9.7-fold higher than in population controls.
- The SNs most often involved the colon/rectum (42%), liver (24%), and stomach (19%).
- A strong radiation dose-response relationship was observed, with an OR of 5.2 (95% CI, 1.7–16.0) for local radiation doses between 10 Gy to 29 Gy and 9.6 (95% CI, 2.6–35.2) for doses of 30 Gy and above, compared with survivors who had not received radiation therapy.
- Chemotherapy alone and combined-modality therapy were associated with a significantly increased risk of developing a GI SN (SIR, 9.1; 95% CI, 2.3–23.6; SIR 29.0; 95% CI, 20.5–39.8, respectively).
- The PanCare Childhood and Adolescent Cancer Survivor Care and Follow-Up Studies (PanCareSurFup) consortium quantified the absolute risks by radiation therapy treatment characteristics in a cohort of 69,450 5-year childhood cancer survivors in Europe. ORs were calculated from a case-control study comprising 143 subsequent colorectal cancers within the cohort of childhood cancer survivors.[92]
- Survivors treated with any abdominopelvic radiation therapy were three times more likely to develop a subsequent colorectal cancer than those who did not receive radiation therapy (OR, 3.1; 95% CI, 1.4–6.6).
- By age 40 years, survivors who were treated with abdominopelvic radiation therapy already have a similar risk of colorectal cancer as individuals aged 50 years in the general population when population-based colorectal cancer screening begins.
- The risk of colorectal cancer increases with abdominopelvic radiation therapy dose. Survivors treated with spinal or whole-abdomen radiation therapy are at higher risk than those treated with radiation to other abdominopelvic fields.
- CCSS investigators reported a 4.6-fold higher risk of GI SNs among their study participants than in the general population (95% CI, 3.4–6.1).[90]
- The SNs most often involved the colon (39%), rectum/anus (16%), liver (18%), and stomach (13%).
- The SIR for colorectal cancer was 4.2 (CI, 2.8–6.3).
- The most prevalent GI SN histology was adenocarcinoma (56%).
- The highest risk of GI SNs was associated with abdominal irradiation (SIR, 11.2; CI, 7.6–16.4), but survivors not exposed to radiation also had a significantly increased risk (SIR, 2.4; CI, 1.4–3.9).
- High-dose procarbazine (RR, 3.2; CI, 1.1–9.4) and platinum drugs (RR, 7.6; CI, 2.3–25.5) independently increased the risk of GI SNs.
- St. Jude Children's Research Hospital investigators observed that the SIR for subsequent colorectal carcinoma was 10.9 (95% CI, 6.6–17.0) compared with U.S. population controls. Investigators also observed the following:[91]
- Incidence of a subsequent colorectal carcinoma increased steeply with advancing attained age, with a 40-year cumulative incidence of 1.4% ± 0.53% among the entire cohort (N = 13,048) and 2.3% ± 0.83% for 5-year survivors.
- Colorectal carcinoma risk increased by 70% with each 10 Gy increase in radiation dose. Increasing radiation volume also increased the risk.
- Treatment with alkylating agent chemotherapy was also associated with an 8.8-fold excess risk of subsequent colorectal carcinoma.
- A multi-institutional prospective study observed that potentially precancerous neoplastic polyps were found in 27.8% of childhood cancer survivors who received radiation to the abdomen/pelvis at least 10 years earlier and who had colonoscopic screening between age 35 and 49 years.[94]
- This polyp prevalence is at least as high as that previously reported for the average-risk population older than 50 years and is similar to the 24% incidence rate for patients with hereditary nonpolyposis colon cancer. Polyp prevalence rates in the general population for people aged 35 to 49 years are unclear.
- A DCOG-LATER record linkage study evaluated the risk of histologically confirmed colorectal adenomas among 5,843 5-year childhood cancer survivors followed for a median of 24.9 years.[95]
- The cumulative incidence of colorectal adenoma by age 45 years was 3.6% among survivors who received abdominal pelvic radiation versus 2.0% for survivors who did not receive abdominal pelvic radiation, versus 1.0% among siblings.
- Factors associated with adenoma risk were abdominal pelvic radiation (HR, 2.1), TBI (HR, 10.6), cisplatin (HR, 2.1 for <480 mg/m2; HR, 3.8 for ≥480 mg/m2), diagnosis of hepatoblastoma (HR, 27.1), and family history of early-onset colorectal cancer (HR, 20.5).
- Procarbazine exposure was also associated with an increased risk among survivors not exposed to abdominal pelvic radiation or TBI (HR, 2.7).
- The PanCareSurFup consortium reported on digestive cancers in a cohort of 69,460 5-year childhood cancer survivors in Europe.[96]
- Survivors of Wilms tumor (SIR, 12.1; 95% CI, 9.6–15.1) and Hodgkin lymphoma (SIR, 7.3; 95% CI, 5.9–9.0) were at the highest risk for GI SMNs.
- By age 55 years, 2.3% of survivors of Wilms tumor and Hodgkin lymphoma developed a secondary colorectal cancer, a rate that is comparable to that of the general population with two or more first-degree relatives affected by GI cancer.
- A nested case-control study examined the rate of colorectal cancer according to large bowel radiation therapy dose and procarbazine dose among 5-year Hodgkin lymphoma survivors who were diagnosed between age 15 and 50 years (only 27% of cases were 15 to 24 years old) at five hospital centers in the Netherlands (diagnosed between 1964 to 2000; median follow-up, 26 years).[97]
- The median interval between Hodgkin lymphoma diagnosis and subsequent colorectal cancer was 25.7 years (range, 18.2–31.6 years).
- Treatment with subdiaphragmatic radiation therapy (RR, 2.4; 95% CI, 1.4–4.1) and more than 8.4 g/m2 of procarbazine (RR, 2.5; 95% CI, 1.3–5.0) were associated with increased rates of colorectal cancer on univariable analysis.
- Colorectal cancer rate increased linearly with mean radiation therapy dose to the whole large bowel and dose to the affected bowel segment. The dose response became steeper with higher doses of procarbazine and increased 1.2-fold (95% CI, 1.1–1.3) for each 1 g/m2 increase in procarbazine.
Oral cancers
The PanCareSurFup consortium reported on risks of oral second primary neoplasms (validated through pathology reports) in a cohort of 69,460 5-year childhood cancer survivors in Europe.[98]
- Oral second primary neoplasms (n = 145; 64 salivary gland, 38 tongue, 20 pharynx, 2 lip, and 21 other) developed in 143 survivors at a median age of 32 years. This represents a fivefold excess risk compared with that expected in the general population.
- Childhood cancer diagnostic groups at greatest risk for an oral second primary neoplasm included leukemia (SIR, 19.2; 95% CI, 14.6–25.2), bone sarcoma (SIR, 6.4; 95% CI, 3.7–11.0), Hodgkin lymphoma (SIR, 6.2; 95% CI, 3.9–9.9), and soft tissue sarcoma (SIR, 5.0; 95% CI, 3.0–8.5).
- Observed specific treatment associations with oral second primary neoplasms included radiation therapy and salivary gland neoplasms (SIR, 33; 95% CI, 25.3–44.5) and chemotherapy (any exposure) and tongue neoplasms (SIR, 15.9; 95% CI, 10.6–23.7).
- Data were not available to assess the contributions of health behaviors (smoking, alcohol intake) and human papillomavirus (HPV) infection status to the development of oral second primary neoplasms.
Urogenital cancers
Development of subsequent primary urogenital cancers in childhood and adolescent cancer survivors is rare.
Using SEER data of 43,991 patients (aged <20 years) diagnosed with a first primary cancer from 1975 to 2016, the risk of urinary system cancer was higher for both females (SIR, 5.18; 95% CI, 3.65–7.14) and males (SIR, 2.80; 95% CI, 1.94–3.92), compared with the general population.[99]
- Females were more likely than males to develop a subsequent urinary system cancer (SIR, 1.86; 95% CI, 1.13–3.03) and kidney cancer (SIR, 1.97; 95% CI, 1.11–3.53).
- Females with any first cancer had higher risks than the general population for developing cancers of the corpus uteri (SIR, 2.32; 95% CI, 1.49–3.45) and vulva (SIR, 4.27; 95% CI, 1.38–9.95).
Renal carcinoma
Consistent with reports among survivors of adult-onset cancer, an increased risk of renal carcinoma has been observed in survivors of childhood cancer.[29,100,101] Underlying genetic predisposition may also play a role in the risk of developing renal carcinomas because rare cases of renal carcinoma have been observed in children with tuberous sclerosis.[100] Cases of secondary renal carcinoma associated with Xp11.2 translocations and TFE3 gene fusions have also been reported and suggest that cytotoxic chemotherapy may contribute to renal carcinogenesis.[102,103,104]
Evidence (excess risk of renal carcinoma):
- CCSS investigators reported a significant excess of subsequent renal carcinoma among 14,358 5-year survivors in the cohort (SIR, 8.0; 95% CI, 5.2–11.7) compared with the general population.[100]
- The reported overall absolute excess risk of 8.4 per 105 person-years indicates that these cases are relatively rare. Highest risk was observed among the following:
- Neuroblastoma survivors (SIR, 85.8; 95% CI, 38.4–175.2).[100] Radiation has been hypothesized to predispose children with high-risk neuroblastoma to renal carcinoma.[105]
- Those treated with renal-directed radiation therapy of 5 Gy or higher (RR, 3.8; 95% CI, 1.6–9.3).[100]
- Those treated with platinum-based chemotherapy (RR, 3.5; 95% CI, 1.0–11.2).[100]
- The reported overall absolute excess risk of 8.4 per 105 person-years indicates that these cases are relatively rare. Highest risk was observed among the following:
Human Papillomavirus (HPV)–Associated Malignancies
Evidence (HPV-associated SMNs):
- A CCSS study evaluated the occurrence of cancer types in which HPV is an established etiologic risk factor. The study included 24,363 childhood cancer survivors who were a median of 21 years from diagnosis.[106]
- The 30-year cumulative incidence of an HPV-associated cancer was 0.3% (95% CI, 0.2%–0.4%), reflecting an almost threefold excess risk (SIR, 2.86; 95% CI, 2.05–4.00) to that of the general population.
- Male and female cancer survivors had an elevated risk of HPV-associated oropharyngeal (SIR in males, 4.06; SIR in females, 8.44) and anorectal (SIR in males, 13.56; SIR in females, 9.16) SMNs. However, females were not at increased risk of cervical or vulvar cancers, compared with the general population.
- Independent risk factors for HPV-associated cancers identified by multivariable modeling included male sex (vs. females: relative SIR, 1.99; 95% CI, 1.00–3.94); head, neck, and pelvic radiation therapy doses higher than 30 Gy (vs. none: relative SIR, 2.35; 95% CI, 1.11–4.97); and cisplatin-equivalent doses higher than 400 mg/m2 (vs. none: relative SIR, 4.51; 95% CI, 1.78–11.43).
- A population-based study used Surveillance, Epidemiology, and End Results (SEER) registry data to evaluate risk factors and trends for HPV-associated SMNs among 374,408 adolescent and young adult (AYA) patients (11% were aged 15–24 years, 28% were aged 25–34 years, and 61% were aged 35–44 years at diagnosis). The patients were diagnosed between 1976 and 2015.[107]
- The incidence of HPV-associated SMNs declined over the study period, and the overall incidence of HPV-associated SMNs among AYA cancer survivors was low, affecting only 0.4% of survivors.
- Risk of any HPV-associated SMN was increased by 70% for AYA survivors (SIR, 1.70; 95% CI, 1.61–1.79) and 117% for oropharyngeal cancer (SIR, 2.17; 95% CI, 2.00–2.35), compared with the general population.
- Cervical cancer risk was overall lower in survivors (SIR, 0.85; 95% CI, 0.76–0.95), but Hispanic AYA survivors had a significant increase in cervical cancer (SIR, 1.46; 95% CI, 1.01–2.06).
- Among survivors with HPV-related first cancers, prior chemotherapy and radiation therapy were associated with any HPV-related SMN. However, those therapies were not associated with HPV-related SMNs among survivors whose first cancers were not HPV related.
Survival Outcomes After SNs
Outcome after the diagnosis of an SN is variable, as treatment for some histological subtypes may be compromised if childhood cancer therapy included cumulative doses of agents and modalities at the threshold of tissue tolerance.
Using data from the SEER Program, individuals younger than 60 years with first primary malignancies (n = 1,332,203) were compared with childhood cancer survivors (n = 1,409) who had a second primary malignancy.[108]
- Survivors of childhood cancer diagnosed with a second primary malignancy experienced poorer overall survival than did their peers without a history of cancer (HR, 1.86; 95% Cl, 1.72–2.02) after the study had accounted for cancer type, age, sex, race, and decade of diagnosis.
- A history of childhood cancer was consistently associated with a twofold to threefold increased risk of death for the most diagnosed second primary malignancies, including breast cancer, thyroid cancer, AML, brain cancer, melanoma, bone cancer, and soft tissue sarcoma.
In a study of female participants in the CCSS who were subsequently diagnosed with breast cancer (n = 274) and matched to a control group of women (n = 1,095) with de novo breast cancer, survivors of childhood cancer were found to have elevated mortality rates (HR, 2.2; 95% CI, 1.7–3.0) even after adjusting for breast cancer treatment.[54]
- Survivors were five times more likely to die as a result of other health-related causes, including other SMNs and cardiovascular or pulmonary disease (HR, 5.5; 95% CI, 3.4–9.0).
- The cumulative incidence of a second asynchronous breast cancer was elevated significantly compared with controls (at 5 years, 8.0% among childhood cancer survivors vs. 2.7% among controls; P < .001).
Subsequent Neoplasms and Genetic Susceptibility
Literature clearly supports the role of chemotherapy and radiation therapy in the development of SNs. However, interindividual variability exists, suggesting that genetic variation has a role in susceptibility to genotoxic exposures, or that genetic susceptibility syndromes confer an increased risk of cancer, such as Li-Fraumeni syndrome.[109,110] In a population-based Swiss Childhood Cancer Survivor Study, cancer predisposition syndromes were associated with a high risk of second primary neoplasms before the age of 21 years and represented the most important risk factor (HR, 7.8; 95% CI, 4.8–12.7) for developing a second primary cancer.[111]
Previous studies have demonstrated that childhood cancer survivors with a family history of Li-Fraumeni syndrome in particular, or a family history of cancer, carry an increased risk of developing an SN.[112,113] A prospective registry followed 480 individuals with pathogenic or likely pathogenic germline TP53 variants.[114] Individuals who developed a first cancer were monitored for the development of a second malignant neoplasm. Among individuals who were younger than 17 years at the time of diagnosis of their first cancer, 50% developed a second cancer within 20 years.
The risk of SNs could potentially be modified by variants in high-penetrance genes that lead to these serious genetic diseases (e.g., Li-Fraumeni syndrome).[113] However, the attributable risk is expected to be very small because of the extremely low prevalence of variants in high-penetrance genes.
Likewise, children with neurofibromatosis type 1 (NF1) who develop a primary tumor are at an increased risk of SNs compared with childhood cancer survivors without NF1. Treatment with radiation, but not alkylating agents, increases the risk of SNs in survivors with NF1.[115] SNs represent a major contributor to excess mortality in adult survivors of childhood glioma with NF1.[116] These survivors developed late-onset (>5 years from diagnosis) SMNs at four times the rate of glioma survivors without NF1 (4.02; range, 2.12–7.62). The 30-year, all-cause late mortality rate was 46.3% (95% CI, 23.9%–62.2%) in glioma survivors with NF1, compared with 18% (95% CI, 16.1%–20.0%) in glioma survivors without NF1. The most common causes of death among survivors with NF1 and glioma were SNs.
Table 1 summarizes the spectrum of neoplasms, affected genes, and Mendelian mode of inheritance of selected syndromes of inherited cancer predisposition.
| Syndrome | Major Tumor Types | Affected Gene | Mode of Inheritance |
|---|---|---|---|
| AML = acute myeloid leukemia; MDS = myelodysplastic syndromes; WAGR = Wilms tumor, aniridia, genitourinary abnormalities, and range of developmental delays. | |||
| a Adapted from Strahm et al.[117] | |||
| b Dominant in a fraction of patients, spontaneous variants can occur. | |||
| Adenomatous polyposis of the colon | Colon, hepatoblastoma, intestinal cancers, stomach, thyroid cancer | APC | Dominant |
| Ataxia-telangiectasia | Leukemia, lymphoma | ATM | Recessive |
| Beckwith-Wiedemann syndrome | Adrenal carcinoma, hepatoblastoma, rhabdomyosarcoma, Wilms tumor | CDKN1C,NSD1 | Dominant |
| Bloom syndrome | Leukemia, lymphoma, skin cancer | BLM | Recessive |
| Diamond-Blackfan anemia | Colon cancer, osteogenic sarcoma, AML/MDS | RPS19and otherRPgenes | Dominant, spontaneousb |
| Fanconi anemia | Gynecological tumors, leukemia, squamous cell carcinoma | FANCA, FANCB, FANCC, FANCD2, FANCE, FANCF, FANCG | Recessive |
| Juvenile polyposis syndrome | Gastrointestinal tumors | SMAD4 | Dominant |
| Li-Fraumeni syndrome | Adrenocortical carcinoma, brain tumor, breast carcinoma, leukemia, osteosarcoma, soft tissue sarcoma | TP53 | Dominant |
| Multiple endocrine neoplasia 1 | Pancreatic islet cell tumor, parathyroid adenoma, pituitary adenoma | MEN1 | Dominant |
| Multiple endocrine neoplasia 2 | Medullary thyroid carcinoma, pheochromocytoma | RET | Dominant |
| Neurofibromatosis type 1 | Neurofibroma, optic pathway glioma, peripheral nerve sheath tumor | NF1 | Dominant |
| Neurofibromatosis type 2 | Vestibular schwannoma | NF2 | Dominant |
| Nevoid basal cell carcinoma syndrome | Basal cell carcinoma, medulloblastoma | PTCH | Dominant |
| Peutz-Jeghers syndrome | Intestinal cancers, ovarian carcinoma, pancreatic carcinoma | STK11 | Dominant |
| Retinoblastoma | Osteosarcoma, retinoblastoma | RB1 | Dominant |
| Tuberous sclerosis | Hamartoma, renal angiomyolipoma, renal cell carcinoma | TSC1,TSC2 | Dominant |
| von Hippel-Lindau syndrome | Hemangioblastoma, pheochromocytoma, renal cell carcinoma, retinal and central nervous system tumors | VHL | Dominant |
| WAGR syndrome | Gonadoblastoma, Wilms tumor | WT1 | Dominant |
| Wilms tumor syndrome | Wilms tumor | WT1 | Dominant |
| Xeroderma pigmentosum | Leukemia, melanoma | XPA, XPB, XPC, XPD, XPE, XPF, XPG, POLH | Recessive |
The McGill Interactive Pediatric OncoGenetic Guidelines (MIPOGG) tool identifies children with cancer who have an increased likelihood of having a cancer predisposition syndrome. This tool guides clinicians through a series of yes or no questions, and it generates a recommendation for or against genetic evaluation.[118,119]
- In a population-based, nested, case-control study, the MIPOGG tool identified survivors who were at increased risk of developing SMNs, after controlling for radiation and chemotherapy exposures (HR, 1.53; 95% CI, 1.06–2.19).
- SMN prediction was superior in survivors of CNS and solid tumor neoplasms and in survivors who were not irradiated during treatment of their primary malignancy.
- Use of the MIPOGG tool in pediatric oncology patients, at diagnosis or in survivorship follow-up, may help prioritize those who should undergo genetic evaluation.
Drug-metabolizing enzymes and DNA repair polymorphisms
The interindividual variability in risk of SNs is more likely related to common polymorphisms in low-penetrance genes that regulate the availability of active drug metabolites or are responsible for DNA repair. Gene-environment interactions may magnify subtle functional differences resulting from genetic variations.
In related research, SJLIFE investigators evaluated cancer treatments and pathogenic germline variants in 127 genes from six major DNA repair pathways to identify childhood cancer survivors at an increased risk of SNs.[120]
- Among 4,402 survivors who underwent whole-genome sequencing, 495 (11.2%) developed 1,269 SNs.
- Among 508 survivors (11.5%), 538 pathogenic germline variants were identified in 98 DNA repair pathways (e.g., POLG, MUTYH, ERCC2, and BRCA2).
The following three groups were identified to have an elevated risk of SNs:
- Female survivors with variants in homologous recombination genes who were treated with high doses (≥20 Gy) of chest radiation (RR, 4.4; 95% CI, 1.6–12.4) or a cumulative dose of anthracyclines in the second or third tertile (RR, 4.4; 95% CI, 1.7–11.4) had a significantly increased risk of breast cancer.
- Survivors with variants in homologous recombination genes who received alkylating agent doses in the third tertile had an increased rate of subsequent sarcomas (RR, 14.9; 95% CI, 4.0–38.0).
- Survivors with variants in nucleotide excision repair genes who were treated with neck radiation (≥30 Gy) had an increased risk of subsequent thyroid cancer (RR, 12.9; 95% CI, 1.6–46.6).
Drug-metabolizing enzymes
Metabolism of genotoxic agents occurs in two phases.
- Phase I involves activation of substrates into highly reactive electrophilic intermediates that can damage DNA, a reaction principally performed by the cytochrome p450 (CYP) family of enzymes.
- Phase II enzymes (conjugation) function to inactivate genotoxic substrates. The phase II proteins comprise the glutathione S-transferase (GST) enzymes, NAD(P)H:quinone oxidoreductase-1 (NQO1) enzyme, and others.
The balance between the two sets of enzymes is critical to the cellular response to xenobiotics; for example, high activity of a phase I enzyme and low activity of a phase II enzyme can result in DNA damage.
DNA repair polymorphisms
DNA repair mechanisms protect somatic cells from variants in tumor suppressor genes and oncogenes that can lead to cancer initiation and progression. An individual's DNA repair capacity appears to be genetically determined.[121] A number of DNA repair genes contain polymorphic variants, resulting in large interindividual variations in DNA repair capacity.[121] Evaluation of the contribution of polymorphisms influencing DNA repair to the risk of SN represents an active area of research.
Polygenic risk
Survivors of childhood cancer are at an increased risk of subsequent cancers attributable to the late effects of radiation therapy and other treatment exposures. To better understand the impact of genetic predisposition on this risk, several studies have examined radiation-related cancers and chemotherapy only–related cancers.
Investigators combined genotype data for 11,220 5-year survivors from the CCSS and SJLIFE cohort study. They conducted a comprehensive investigation of general population, cancer-specific polygenic risk scores (PRS) derived from genome-wide association study findings. The study aimed to identify whether the PRS were associated with subsequent cancer risk among survivors of childhood cancer, after controlling for treatment exposure and nongenetic risk factors. They also quantified joint associations between radiation therapy and PRS to understand the potential interplay between genetic and treatment risk factors.[122]
- In survivors of predominantly European ancestry, standardized PRS were significantly associated with the risk of subsequent BCCs (OR, 1.37; n = 958), female breast cancers (OR, 1.42; n = 360), thyroid cancers (OR, 1.48; n = 259), squamous cell carcinomas (OR, 1.20; n = 127), and melanomas (OR, 1.60; n = 103). The association between colorectal cancer PRS and subsequent colorectal cancer risk did not reach the threshold for statistical significance (OR, 1.19; n = 67).
- Childhood cancer survivors with a higher PRS and who received radiation therapy had more-than-additive increased risks of developing BCCs, breast cancers, and thyroid cancers.
- For female survivors who were exposed to chest radiation therapy (>10 Gy), those with high PRS had an increased cumulative incidence of subsequent breast cancer by age 50 years, compared with those with low PRS.
With the decreased use of radiation therapy, it has become important to define the role of genetic susceptibility in chemotherapy-related SMNs. SJLIFE cohort study investigators evaluated treatment-related SMNs among long-term survivors of childhood cancer. An externally validated 179-variant PRS associated with risks of common adult-onset cancers in the general population was calculated for each survivor.[123]
- The most frequent SMNs developing in 1,594 survivors included BCC (n = 822), breast cancer (n = 235), and thyroid cancer (n = 221).
- SMN risk associations with the PRS were extremely modest in survivors with European ancestry who were exposed to radiation therapy (HR, 1.22; n = 4,630).
- Among survivors with European ancestry who did not receive radiation therapy (n = 4,322), the increase in 30-year SMN cumulative incidence and HRs comparing top and bottom PRS quintiles was statistically significant for those treated with alkylating agents (17% vs. 6%; HR, 2.46; P < .01), anthracyclines (20% vs. 8%; HR, 2.86; P < .001), epipodophyllotoxins (23% vs. 1%; HR, 12.20; P < .001), or platinums (46% vs. 7%; HR, 8.58; P < .01).
- Among survivors with African ancestry who did not receive radiation therapy (n = 414), the PRS also significantly predicted epipodophyllotoxin-related SMN risk. The greatest improvements in risk prediction were for survivors who were exposed to epipodophyllotoxins (HR, 2.68; P < .01).
Screening and Follow-Up for Subsequent Neoplasms
Vigilant screening is important for childhood cancer survivors at risk.[124] Because of the relatively small size of the pediatric cancer survivor population and the prevalence and time to onset of therapy-related complications, undertaking clinical studies to assess the impact of screening recommendations on the morbidity and mortality associated with the late effect is not feasible.
Well-conducted studies of large populations of childhood cancer survivors have provided compelling evidence linking specific therapeutic exposures and late effects. This evidence has been used by several national and international cooperative groups (Scottish Collegiate Guidelines Network, Children's Cancer and Leukaemia Group, Children's Oncology Group [COG], DCOG) to develop consensus-based clinical practice guidelines to increase awareness and standardize the immediate care needs of medically vulnerable childhood cancer survivors.[125]
All pediatric cancer survivor health screening guidelines employ a hybrid approach that is both evidence-based (using established associations between therapeutic exposures and late effects to identify high-risk categories) and grounded in the collective clinical experience of experts (matching the magnitude of the risk with the intensity of the screening recommendations). The screening recommendations in these guidelines represent a statement of consensus from a panel of experts in the late effects of pediatric cancer treatment.[124,125]
The COG Guidelines for malignant SNs indicate that certain high-risk populations of childhood cancer survivors merit heightened surveillance because of predisposing host, behavioral, or therapeutic factors.[124]
- Screening for leukemia: MDS-pCT or AML-pCT usually manifests within 10 years after exposure. Recommendations include monitoring with history and physical examination for signs and symptoms of pancytopenia for 10 years after exposure to alkylating agents or topoisomerase II inhibitors.
- Screening after radiation exposure: Most other SNs are associated with radiation exposure and usually manifest more than 10 years after exposure. Screening recommendations include careful annual physical examination of the skin and exposed (often underlying) tissues in the radiation field.
Specific comments about screening for more common radiation-associated SNs are as follows:
- Screening for early-onset skin cancer: Annual dermatological examination focusing on skin lesions and pigmented nevi in the radiation field is recommended. Survivors are counseled about the following:
- Increased risk of skin cancer.
- Potential exacerbation of risk through tanning.
- Benefits of adhering to behaviors to protect the skin from excessive UV radiation exposure.
- Screening for early-onset breast cancer: Because outcome after breast cancer is directly linked to stage at diagnosis, close surveillance that results in early diagnosis may improve survival.[126] Several pediatric cancer groups have endorsed the recommendation for early (before population breast cancer screening) initiation of breast cancer surveillance using mammography, breast MRI, or both imaging modalities in young women who were treated with chest irradiation.[126]
Mammography, the most widely accepted screening tool for breast cancer in the general population, may not be the ideal screening tool by itself for radiation-related breast cancers occurring in relatively young women with dense breasts. On the basis of research among young women with inherited susceptibility to breast cancer, dual-imaging modalities may enhance early detection related to the higher sensitivity of MRI in detecting lesions in premenopausal dense breasts and the superiority of mammography in identifying ductal carcinoma in situ;[127,128,129] therefore, the American Cancer Society recommends including adjunct screening with MRI.[130] The high sensitivity and specificity in detecting early-stage lesions with dual-imaging surveillance is offset by a substantial rate of additional investigations attributable to false-positive results.[129]
Many clinicians are concerned about potential harms related to radiation exposure associated with annual mammography in these young women. In this regard, it is important to consider that the estimated mean breast dose with contemporary standard two-view screening mammograms is about 3.85 mGy to 4.5 mGy.[131,132,133] Thus, 15 additional surveillance mammograms from age 25 to 39 years would increase the total radiation exposure in a woman treated with 20 Gy of chest radiation to 20.05775 Gy. The benefits of detection of early breast cancer lesions in high-risk women must be balanced by the risk predisposed by a 0.3% additional radiation exposure.
To keep young women engaged in breast health surveillance, the COG Guideline recommends the following for females who received a radiation dose of 10 Gy or higher to the mantle, mediastinal, whole lung, and axillary fields:
- Monthly breast self-examination beginning at puberty.
- Annual clinical breast examinations beginning at puberty until age 25 years.
- A clinical breast examination every 6 months, with annual mammograms and MRIs beginning 8 years after radiation therapy or at age 25 years (whichever occurs later).
The risk of breast cancer in patients who received less than 10 Gy of radiation with potential impact to the breast is of a lower magnitude compared with those who received 10 Gy or higher. Monitoring of patients treated with less than 10 Gy of radiation with potential impact to the breast is determined on an individual basis after a discussion with the provider regarding the benefits and risk/harms of screening. If a decision is made to screen, the recommendations for women exposed to 10 Gy or higher are used.
- Screening for thyroid cancer: Surveillance recommendations for thyroid cancer among survivors treated with radiation therapy to the thyroid gland vary a great deal. Consensus recommendations for surveillance were developed by the International Guidelines Harmonization Group (IGHG) with the PanCareSurFup consortium. Ultimately, neither of the two surveillance strategies, thyroid ultrasonography and neck palpation, was demonstrated to be superior. This finding highlights the need for shared decision-making between the medical provider and patient.[134]
- Screening for subsequent CNS neoplasms: The IGHG identified a paucity of high-quality evidence for CNS screening. The group determined there was insufficient evidence to establish whether early CNS neoplasm detection results in reduced morbidity and/or mortality. Therefore, a recommendation was not made for or against MRI surveillance. Shared decision-making between the medical provider and survivor is recommended to formulate a screening plan.[68]
- Screening for early-onset colorectal cancer: Screening of those at risk of early-onset colorectal cancer (i.e., radiation doses of 20 Gy or higher to the abdomen, pelvis, or spine) includes colonoscopy every 5 years or multitarget stool DNA test every 3 years beginning at age 30 years or 5 years after radiation therapy (whichever occurs later). For more information, see the COG Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers.
- Screening for early-onset skin cancer: Annual dermatological examination focusing on skin lesions and pigmented nevi in the radiation field is recommended. Survivors are counseled about the following:
References:
- Mertens AC, Liu Q, Neglia JP, et al.: Cause-specific late mortality among 5-year survivors of childhood cancer: the Childhood Cancer Survivor Study. J Natl Cancer Inst 100 (19): 1368-79, 2008.
- Friedman DL, Whitton J, Leisenring W, et al.: Subsequent neoplasms in 5-year survivors of childhood cancer: the Childhood Cancer Survivor Study. J Natl Cancer Inst 102 (14): 1083-95, 2010.
- Turcotte LM, Whitton JA, Friedman DL, et al.: Risk of Subsequent Neoplasms During the Fifth and Sixth Decades of Life in the Childhood Cancer Survivor Study Cohort. J Clin Oncol 33 (31): 3568-75, 2015.
- Turcotte LM, Liu Q, Yasui Y, et al.: Temporal Trends in Treatment and Subsequent Neoplasm Risk Among 5-Year Survivors of Childhood Cancer, 1970-2015. JAMA 317 (8): 814-824, 2017.
- Stiller CA, Bunch KJ, Bayne AM, et al.: Subsequent cancers within 5 years from initial diagnosis of childhood cancer. Patterns and risks in the population of Great Britain. Pediatr Blood Cancer 70 (5): e30258, 2023.
- Withrow DR, Anderson H, Armstrong GT, et al.: Pooled Analysis of Meningioma Risk Following Treatment for Childhood Cancer. JAMA Oncol 8 (12): 1756-1764, 2022.
- Armstrong GT, Liu W, Leisenring W, et al.: Occurrence of multiple subsequent neoplasms in long-term survivors of childhood cancer: a report from the childhood cancer survivor study. J Clin Oncol 29 (22): 3056-64, 2011.
- van Eggermond AM, Schaapveld M, Lugtenburg PJ, et al.: Risk of multiple primary malignancies following treatment of Hodgkin lymphoma. Blood 124 (3): 319-27; quiz 466, 2014.
- Bowers DC, Moskowitz CS, Chou JF, et al.: Morbidity and Mortality Associated With Meningioma After Cranial Radiotherapy: A Report From the Childhood Cancer Survivor Study. J Clin Oncol 35 (14): 1570-1576, 2017.
- Kok JL, Teepen JC, van Leeuwen FE, et al.: Risk of benign meningioma after childhood cancer in the DCOG-LATER cohort: contributions of radiation dose, exposed cranial volume, and age. Neuro Oncol 21 (3): 392-403, 2019.
- Verbruggen LC, Kok JL, Teepen JC, et al.: Clinical characteristics of subsequent histologically confirmed meningiomas in long-term childhood cancer survivors: A Dutch LATER study. Eur J Cancer 150: 240-249, 2021.
- Turcotte LM, Liu Q, Yasui Y, et al.: Chemotherapy and Risk of Subsequent Malignant Neoplasms in the Childhood Cancer Survivor Study Cohort. J Clin Oncol 37 (34): 3310-3319, 2019.
- Teepen JC, van Leeuwen FE, Tissing WJ, et al.: Long-Term Risk of Subsequent Malignant Neoplasms After Treatment of Childhood Cancer in the DCOG LATER Study Cohort: Role of Chemotherapy. J Clin Oncol 35 (20): 2288-2298, 2017.
- Wang Z, Wilson CL, Easton J, et al.: Genetic Risk for Subsequent Neoplasms Among Long-Term Survivors of Childhood Cancer. J Clin Oncol 36 (20): 2078-2087, 2018.
- Allodji RS, Hawkins MM, Bright CJ, et al.: Risk of subsequent primary leukaemias among 69,460 five-year survivors of childhood cancer diagnosed from 1940 to 2008 in Europe: A cohort study within PanCareSurFup. Eur J Cancer 117: 71-83, 2019.
- Allodji RS, Tucker MA, Hawkins MM, et al.: Role of radiotherapy and chemotherapy in the risk of leukemia after childhood cancer: An international pooled analysis. Int J Cancer 148 (9): 2079-2089, 2021.
- Ghosh T, Hyun G, Dhaduk R, et al.: Late subsequent leukemia after childhood cancer: A report from the Childhood Cancer Survivor Study (CCSS). Cancer Med 13 (20): e70086, 2024.
- Bhatia S, Yasui Y, Robison LL, et al.: High risk of subsequent neoplasms continues with extended follow-up of childhood Hodgkin's disease: report from the Late Effects Study Group. J Clin Oncol 21 (23): 4386-94, 2003.
- Nottage K, Lanctot J, Li Z, et al.: Long-term risk for subsequent leukemia after treatment for childhood cancer: a report from the Childhood Cancer Survivor Study. Blood 117 (23): 6315-8, 2011.
- Khoury JD, Solary E, Abla O, et al.: The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia 36 (7): 1703-1719, 2022.
- Thirman MJ, Larson RA: Therapy-related myeloid leukemia. Hematol Oncol Clin North Am 10 (2): 293-320, 1996.
- Pedersen-Bjergaard J, Philip P: Balanced translocations involving chromosome bands 11q23 and 21q22 are highly characteristic of myelodysplasia and leukemia following therapy with cytostatic agents targeting at DNA-topoisomerase II. Blood 78 (4): 1147-8, 1991.
- Kok JL, Teepen JC, van der Pal HJ, et al.: Incidence of and Risk Factors for Histologically Confirmed Solid Benign Tumors Among Long-term Survivors of Childhood Cancer. JAMA Oncol 5 (5): 671-680, 2019.
- Inskip PD, Sigurdson AJ, Veiga L, et al.: Radiation-Related New Primary Solid Cancers in the Childhood Cancer Survivor Study: Comparative Radiation Dose Response and Modification of Treatment Effects. Int J Radiat Oncol Biol Phys 94 (4): 800-7, 2016.
- Ehrhardt MJ, Howell CR, Hale K, et al.: Subsequent Breast Cancer in Female Childhood Cancer Survivors in the St Jude Lifetime Cohort Study (SJLIFE). J Clin Oncol 37 (19): 1647-1656, 2019.
- Taylor AJ, Little MP, Winter DL, et al.: Population-based risks of CNS tumors in survivors of childhood cancer: the British Childhood Cancer Survivor Study. J Clin Oncol 28 (36): 5287-93, 2010.
- Henderson TO, Whitton J, Stovall M, et al.: Secondary sarcomas in childhood cancer survivors: a report from the Childhood Cancer Survivor Study. J Natl Cancer Inst 99 (4): 300-8, 2007.
- Veiga LH, Holmberg E, Anderson H, et al.: Thyroid Cancer after Childhood Exposure to External Radiation: An Updated Pooled Analysis of 12 Studies. Radiat Res 185 (5): 473-84, 2016.
- Reulen RC, Frobisher C, Winter DL, et al.: Long-term risks of subsequent primary neoplasms among survivors of childhood cancer. JAMA 305 (22): 2311-9, 2011.
- Teepen JC, Kok JL, Kremer LC, et al.: Long-Term Risk of Skin Cancer Among Childhood Cancer Survivors: A DCOG-LATER Cohort Study. J Natl Cancer Inst 111 (8): 845-853, 2019.
- Majhail NS, Brazauskas R, Rizzo JD, et al.: Secondary solid cancers after allogeneic hematopoietic cell transplantation using busulfan-cyclophosphamide conditioning. Blood 117 (1): 316-22, 2011.
- Baker KS, Leisenring WM, Goodman PJ, et al.: Total body irradiation dose and risk of subsequent neoplasms following allogeneic hematopoietic cell transplantation. Blood 133 (26): 2790-2799, 2019.
- Veiga LH, Curtis RE, Morton LM, et al.: Association of Breast Cancer Risk After Childhood Cancer With Radiation Dose to the Breast and Anthracycline Use: A Report From the Childhood Cancer Survivor Study. JAMA Pediatr 173 (12): 1171-1179, 2019.
- Kenney LB, Yasui Y, Inskip PD, et al.: Breast cancer after childhood cancer: a report from the Childhood Cancer Survivor Study. Ann Intern Med 141 (8): 590-7, 2004.
- Moskowitz CS, Chou JF, Wolden SL, et al.: Breast cancer after chest radiation therapy for childhood cancer. J Clin Oncol 32 (21): 2217-23, 2014.
- Henderson TO, Liu Q, Turcotte LM, et al.: Association of Changes in Cancer Therapy Over 3 Decades With Risk of Subsequent Breast Cancer Among Female Childhood Cancer Survivors: A Report From the Childhood Cancer Survivor Study (CCSS). JAMA Oncol : , 2022.
- Schaapveld M, Aleman BM, van Eggermond AM, et al.: Second Cancer Risk Up to 40 Years after Treatment for Hodgkin's Lymphoma. N Engl J Med 373 (26): 2499-511, 2015.
- Travis LB, Hill D, Dores GM, et al.: Cumulative absolute breast cancer risk for young women treated for Hodgkin lymphoma. J Natl Cancer Inst 97 (19): 1428-37, 2005.
- O'Brien MM, Donaldson SS, Balise RR, et al.: Second malignant neoplasms in survivors of pediatric Hodgkin's lymphoma treated with low-dose radiation and chemotherapy. J Clin Oncol 28 (7): 1232-9, 2010.
- Inskip PD, Robison LL, Stovall M, et al.: Radiation dose and breast cancer risk in the childhood cancer survivor study. J Clin Oncol 27 (24): 3901-7, 2009.
- Travis LB, Hill DA, Dores GM, et al.: Breast cancer following radiotherapy and chemotherapy among young women with Hodgkin disease. JAMA 290 (4): 465-75, 2003.
- van Leeuwen FE, Klokman WJ, Stovall M, et al.: Roles of radiation dose, chemotherapy, and hormonal factors in breast cancer following Hodgkin's disease. J Natl Cancer Inst 95 (13): 971-80, 2003.
- Lange JM, Takashima JR, Peterson SM, et al.: Breast cancer in female survivors of Wilms tumor: a report from the national Wilms tumor late effects study. Cancer 120 (23): 3722-30, 2014.
- Wang Y, Ronckers CM, van Leeuwen FE, et al.: Subsequent female breast cancer risk associated with anthracycline chemotherapy for childhood cancer. Nat Med 29 (9): 2268-2277, 2023.
- Henderson TO, Moskowitz CS, Chou JF, et al.: Breast Cancer Risk in Childhood Cancer Survivors Without a History of Chest Radiotherapy: A Report From the Childhood Cancer Survivor Study. J Clin Oncol 34 (9): 910-8, 2016.
- Eisenberg ER, Weiss A, Prakash I, et al.: Surgical Management and Contralateral Breast Cancer Risk in Women with History of Radiation Therapy for Hodgkin Lymphoma: Results from a Population-Based Cohort. Ann Surg Oncol 29 (11): 6673-6680, 2022.
- Moskowitz CS, Ronckers CM, Chou JF, et al.: Development and Validation of a Breast Cancer Risk Prediction Model for Childhood Cancer Survivors Treated With Chest Radiation: A Report From the Childhood Cancer Survivor Study and the Dutch Hodgkin Late Effects and LATER Cohorts. J Clin Oncol 39 (27): 3012-3021, 2021.
- Dores GM, Anderson WF, Beane Freeman LE, et al.: Risk of breast cancer according to clinicopathologic features among long-term survivors of Hodgkin's lymphoma treated with radiotherapy. Br J Cancer 103 (7): 1081-4, 2010.
- Horst KC, Hancock SL, Ognibene G, et al.: Histologic subtypes of breast cancer following radiotherapy for Hodgkin lymphoma. Ann Oncol 25 (4): 848-51, 2014.
- Demoor-Goldschmidt C, Supiot S, Mahé MA, et al.: Clinical and histological features of second breast cancers following radiotherapy for childhood and young adult malignancy. Br J Radiol 91 (1086): 20170824, 2018.
- Castiglioni F, Terenziani M, Carcangiu ML, et al.: Radiation effects on development of HER2-positive breast carcinomas. Clin Cancer Res 13 (1): 46-51, 2007.
- Gaffney DK, Hemmersmeier J, Holden J, et al.: Breast cancer after mantle irradiation for Hodgkin's disease: correlation of clinical, pathologic, and molecular features including loss of heterozygosity at BRCA1 and BRCA2. Int J Radiat Oncol Biol Phys 49 (2): 539-46, 2001.
- Wong SM, Ajjamada L, Weiss AC, et al.: Clinicopathologic features of breast cancers diagnosed in women treated with prior radiation therapy for Hodgkin lymphoma: Results from a population-based cohort. Cancer 128 (7): 1365-1372, 2022.
- Moskowitz CS, Chou JF, Neglia JP, et al.: Mortality After Breast Cancer Among Survivors of Childhood Cancer: A Report From the Childhood Cancer Survivor Study. J Clin Oncol 37 (24): 2120-2130, 2019.
- Yeh JM, Lowry KP, Schechter CB, et al.: Clinical Benefits, Harms, and Cost-Effectiveness of Breast Cancer Screening for Survivors of Childhood Cancer Treated With Chest Radiation : A Comparative Modeling Study. Ann Intern Med 173 (5): 331-341, 2020.
- Vivanco M, Dalle JH, Alberti C, et al.: Malignant and benign thyroid nodules after total body irradiation preceding hematopoietic cell transplantation during childhood. Eur J Endocrinol 167 (2): 225-33, 2012.
- Friedman DN, Goodman PJ, Leisenring WM, et al.: Impact of risk-based therapy on late morbidity and mortality in neuroblastoma survivors: a report from the Childhood Cancer Survivor Study. J Natl Cancer Inst 116 (6): 885-894, 2024.
- Michaelson EM, Chen YH, Silver B, et al.: Thyroid malignancies in survivors of Hodgkin lymphoma. Int J Radiat Oncol Biol Phys 88 (3): 636-41, 2014.
- Sigurdson AJ, Ronckers CM, Mertens AC, et al.: Primary thyroid cancer after a first tumour in childhood (the Childhood Cancer Survivor Study): a nested case-control study. Lancet 365 (9476): 2014-23, 2005 Jun 11-17.
- Clement SC, Lebbink CA, Klein Hesselink MS, et al.: Presentation and outcome of subsequent thyroid cancer among childhood cancer survivors compared to sporadic thyroid cancer: a matched national study. Eur J Endocrinol 183 (2): 169-180, 2020.
- Casey DL, Vogelius IR, Brodin NP, et al.: Risk of Subsequent Neoplasms in Childhood Cancer Survivors After Radiation Therapy: A PENTEC Comprehensive Review. Int J Radiat Oncol Biol Phys 119 (2): 640-654, 2024.
- Hijiya N, Hudson MM, Lensing S, et al.: Cumulative incidence of secondary neoplasms as a first event after childhood acute lymphoblastic leukemia. JAMA 297 (11): 1207-15, 2007.
- Neglia JP, Robison LL, Stovall M, et al.: New primary neoplasms of the central nervous system in survivors of childhood cancer: a report from the Childhood Cancer Survivor Study. J Natl Cancer Inst 98 (21): 1528-37, 2006.
- Faraci M, Morana G, Bagnasco F, et al.: Magnetic resonance imaging in childhood leukemia survivors treated with cranial radiotherapy: a cross sectional, single center study. Pediatr Blood Cancer 57 (2): 240-6, 2011.
- Vinchon M, Leblond P, Caron S, et al.: Radiation-induced tumors in children irradiated for brain tumor: a longitudinal study. Childs Nerv Syst 27 (3): 445-53, 2011.
- Koike T, Yanagimachi N, Ishiguro H, et al.: High incidence of radiation-induced cavernous hemangioma in long-term survivors who underwent hematopoietic stem cell transplantation with radiation therapy during childhood or adolescence. Biol Blood Marrow Transplant 18 (7): 1090-8, 2012.
- Heymer EJ, Hawkins MM, Winter DL, et al.: Risk of subsequent gliomas and meningiomas among 69,460 5-year survivors of childhood and adolescent cancer in Europe: the PanCareSurFup study. Br J Cancer 130 (6): 976-986, 2024.
- Bowers DC, Verbruggen LC, Kremer LCM, et al.: Surveillance for subsequent neoplasms of the CNS for childhood, adolescent, and young adult cancer survivors: a systematic review and recommendations from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Oncol 22 (5): e196-e206, 2021.
- Baliga S, Gallotto S, Bajaj B, et al.: Decade-long disease, secondary malignancy, and brainstem injury outcomes in pediatric and young adult medulloblastoma patients treated with proton radiotherapy. Neuro Oncol 24 (6): 1010-1019, 2022.
- Wong JR, Morton LM, Tucker MA, et al.: Risk of subsequent malignant neoplasms in long-term hereditary retinoblastoma survivors after chemotherapy and radiotherapy. J Clin Oncol 32 (29): 3284-90, 2014.
- Fidler MM, Reulen RC, Winter DL, et al.: Risk of Subsequent Bone Cancers Among 69 460 Five-Year Survivors of Childhood and Adolescent Cancer in Europe. J Natl Cancer Inst 110 (2): , 2018.
- Bright CJ, Hawkins MM, Winter DL, et al.: Risk of Soft-Tissue Sarcoma Among 69 460 Five-Year Survivors of Childhood Cancer in Europe. J Natl Cancer Inst 110 (6): 649-660, 2018.
- Chaussade A, Millot G, Wells C, et al.: Correlation between RB1germline mutations and second primary malignancies in hereditary retinoblastoma patients treated with external beam radiotherapy. Eur J Med Genet 62 (3): 217-223, 2019.
- Kube SJ, Blattmann C, Bielack SS, et al.: Secondary malignant neoplasms after bone and soft tissue sarcomas in children, adolescents, and young adults. Cancer 128 (9): 1787-1800, 2022.
- Schwartz B, Benadjaoud MA, Cléro E, et al.: Risk of second bone sarcoma following childhood cancer: role of radiation therapy treatment. Radiat Environ Biophys 53 (2): 381-90, 2014.
- Bielack SS, Blattmann C, Hassenpflug W, et al.: Osteosarcoma Arising After Ewing Sarcoma or Vice Versa: A Report of 20 Affected Patients from the Cooperative Osteosarcoma Study Group (COSS). Anticancer Res 43 (11): 4975-4981, 2023.
- Henderson TO, Rajaraman P, Stovall M, et al.: Risk factors associated with secondary sarcomas in childhood cancer survivors: a report from the childhood cancer survivor study. Int J Radiat Oncol Biol Phys 84 (1): 224-30, 2012.
- Reulen RC, Winter DL, Diallo I, et al.: Risk Factors for Primary Bone Cancer After Childhood Cancer: A PanCare Childhood and Adolescent Cancer Survivor Care and Follow-Up Studies Nested Case-Control Study. J Clin Oncol 41 (21): 3735-3746, 2023.
- MacCarthy A, Bayne AM, Brownbill PA, et al.: Second and subsequent tumours among 1927 retinoblastoma patients diagnosed in Britain 1951-2004. Br J Cancer 108 (12): 2455-63, 2013.
- Temming P, Arendt M, Viehmann A, et al.: Incidence of second cancers after radiotherapy and systemic chemotherapy in heritable retinoblastoma survivors: A report from the German reference center. Pediatr Blood Cancer 64 (1): 71-80, 2017.
- Kleinerman RA, Schonfeld SJ, Sigel BS, et al.: Bone and Soft-Tissue Sarcoma Risk in Long-Term Survivors of Hereditary Retinoblastoma Treated With Radiation. J Clin Oncol 37 (35): 3436-3445, 2019.
- Thorsness SL, Freites-Martinez A, Marchetti MA, et al.: Nonmelanoma Skin Cancer in Childhood and Young Adult Cancer Survivors Previously Treated With Radiotherapy. J Natl Compr Canc Netw 17 (3): 237-243, 2019.
- Boull C, Chen Y, Im C, et al.: Keratinocyte carcinomas in survivors of childhood cancer: A report from the childhood cancer survivor study. J Am Acad Dermatol 91 (6): 1125-1135, 2024.
- Geller AC, Coroiu A, Keske RR, et al.: Advancing Survivors Knowledge (ASK Study) of Skin Cancer Surveillance After Childhood Cancer: A Randomized Controlled Trial in the Childhood Cancer Survivor Study. J Clin Oncol 41 (12): 2269-2280, 2023.
- Rotz SJ, Stratton K, Leisenring WM, et al.: Melanoma Among Adult Survivors of Childhood Cancer: A Report From the Childhood Cancer Survivor Study. J Clin Oncol 43 (10): 1219-1228, 2025.
- Braam KI, Overbeek A, Kaspers GJ, et al.: Malignant melanoma as second malignant neoplasm in long-term childhood cancer survivors: a systematic review. Pediatr Blood Cancer 58 (5): 665-74, 2012.
- Kleinerman RA, Schonfeld SJ, Abramson DH, et al.: Increased Risk of Skin Cancer in 1,851 Long-Term Retinoblastoma Survivors. J Invest Dermatol 141 (12): 2849-2857.e3, 2021.
- Ghosh T, Chen Y, Dietz AC, et al.: Lung Cancer as a Subsequent Malignant Neoplasm in Survivors of Childhood Cancer. Cancer Epidemiol Biomarkers Prev 30 (12): 2235-2243, 2021.
- van Leeuwen FE, Klokman WJ, Stovall M, et al.: Roles of radiotherapy and smoking in lung cancer following Hodgkin's disease. J Natl Cancer Inst 87 (20): 1530-7, 1995.
- Henderson TO, Oeffinger KC, Whitton J, et al.: Secondary gastrointestinal cancer in childhood cancer survivors: a cohort study. Ann Intern Med 156 (11): 757-66, W-260, 2012.
- Nottage K, McFarlane J, Krasin MJ, et al.: Secondary colorectal carcinoma after childhood cancer. J Clin Oncol 30 (20): 2552-8, 2012.
- Heymer EJ, Jóźwiak K, Kremer LC, et al.: Cumulative Absolute Risk of Subsequent Colorectal Cancer After Abdominopelvic Radiotherapy Among Childhood Cancer Survivors: A PanCareSurFup Study. J Clin Oncol 42 (3): 336-347, 2024.
- Tukenova M, Diallo I, Anderson H, et al.: Second malignant neoplasms in digestive organs after childhood cancer: a cohort-nested case-control study. Int J Radiat Oncol Biol Phys 82 (3): e383-90, 2012.
- Daly PE, Samiee S, Cino M, et al.: High prevalence of adenomatous colorectal polyps in young cancer survivors treated with abdominal radiation therapy: results of a prospective trial. Gut 66 (10): 1797-1801, 2017.
- Teepen JC, Kok JL, van Leeuwen FE, et al.: Colorectal Adenomas and Cancers After Childhood Cancer Treatment: A DCOG-LATER Record Linkage Study. J Natl Cancer Inst 110 (7): 758-767, 2018.
- Reulen RC, Wong KF, Bright CJ, et al.: Risk of digestive cancers in a cohort of 69 460 five-year survivors of childhood cancer in Europe: the PanCareSurFup study. Gut : , 2020.
- Geurts YM, Shakir R, Ntentas G, et al.: Association of Radiation and Procarbazine Dose With Risk of Colorectal Cancer Among Survivors of Hodgkin Lymphoma. JAMA Oncol 9 (4): 481-489, 2023.
- Sunguc C, Hawkins MM, Winter DL, et al.: Risk of subsequent primary oral cancer in a cohort of 69,460 5-year survivors of childhood and adolescent cancer in Europe: the PanCareSurFup study. Br J Cancer 128 (1): 80-90, 2023.
- Liu JJ, De Vivo I, Wu CY, et al.: Subsequent primary urogenital cancers among childhood and adolescent cancer survivors in the United States. Urol Oncol 40 (2): 65.e11-65.e18, 2022.
- Wilson CL, Ness KK, Neglia JP, et al.: Renal carcinoma after childhood cancer: a report from the childhood cancer survivor study. J Natl Cancer Inst 105 (7): 504-8, 2013.
- de Vathaire F, Scwhartz B, El-Fayech C, et al.: Risk of a Second Kidney Carcinoma Following Childhood Cancer: Role of Chemotherapy and Radiation Dose to Kidneys. J Urol 194 (5): 1390-5, 2015.
- Hedgepeth RC, Zhou M, Ross J: Rapid development of metastatic Xp11 translocation renal cell carcinoma in a girl treated for neuroblastoma. J Pediatr Hematol Oncol 31 (8): 602-4, 2009.
- Argani P, Laé M, Ballard ET, et al.: Translocation carcinomas of the kidney after chemotherapy in childhood. J Clin Oncol 24 (10): 1529-34, 2006.
- Ma J, Pan C, Yin M: Translocation Renal Cell Carcinoma in a Child Previously Treated for Infantile Fibrosarcoma. Pediatr Dev Pathol 21 (4): 418-422, 2018 Jul-Aug.
- Fleitz JM, Wootton-Gorges SL, Wyatt-Ashmead J, et al.: Renal cell carcinoma in long-term survivors of advanced stage neuroblastoma in early childhood. Pediatr Radiol 33 (8): 540-5, 2003.
- Henderson TO, Fowler BW, Hamann HA, et al.: Subsequent malignant neoplasms in the Childhood Cancer Survivor Study: Occurrence of cancer types in which human papillomavirus is an established etiologic risk factor. Cancer 128 (2): 373-382, 2022.
- Ou JY, Bennion N, Parker K, et al.: Risk Factors and Trends for HPV-Associated Subsequent Malignant Neoplasms among Adolescent and Young Adult Cancer Survivors. Cancer Epidemiol Biomarkers Prev 32 (5): 625-633, 2023.
- Brown AL, Arroyo VM, Agrusa JE, et al.: Survival disparities for second primary malignancies diagnosed among childhood cancer survivors: A population-based assessment. Cancer 125 (20): 3623-3630, 2019.
- Archer NM, Amorim RP, Naves R, et al.: An Increased Risk of Second Malignant Neoplasms After Rhabdomyosarcoma: Population-Based Evidence for a Cancer Predisposition Syndrome? Pediatr Blood Cancer 63 (2): 196-201, 2016.
- Wang X, Sun CL, Hageman L, et al.: Clinical and Genetic Risk Prediction of Subsequent CNS Tumors in Survivors of Childhood Cancer: A Report From the COG ALTE03N1 Study. J Clin Oncol 35 (32): 3688-3696, 2017.
- Waespe N, Belle FN, Redmond S, et al.: Cancer predisposition syndromes as a risk factor for early second primary neoplasms after childhood cancer - A national cohort study. Eur J Cancer 145: 71-80, 2021.
- Andersson A, Enblad G, Tavelin B, et al.: Family history of cancer as a risk factor for second malignancies after Hodgkin's lymphoma. Br J Cancer 98 (5): 1001-5, 2008.
- Hisada M, Garber JE, Fung CY, et al.: Multiple primary cancers in families with Li-Fraumeni syndrome. J Natl Cancer Inst 90 (8): 606-11, 1998.
- de Andrade KC, Khincha PP, Hatton JN, et al.: Cancer incidence, patterns, and genotype-phenotype associations in individuals with pathogenic or likely pathogenic germline TP53 variants: an observational cohort study. Lancet Oncol 22 (12): 1787-1798, 2021.
- Bhatia S, Chen Y, Wong FL, et al.: Subsequent Neoplasms After a Primary Tumor in Individuals With Neurofibromatosis Type 1. J Clin Oncol 37 (32): 3050-3058, 2019.
- de Blank P, Li N, Fisher MJ, et al.: Late morbidity and mortality in adult survivors of childhood glioma with neurofibromatosis type 1: report from the Childhood Cancer Survivor Study. Genet Med 22 (11): 1794-1802, 2020.
- Strahm B, Malkin D: Hereditary cancer predisposition in children: genetic basis and clinical implications. Int J Cancer 119 (9): 2001-6, 2006.
- Cullinan N, Schiller I, Di Giuseppe G, et al.: Utility of a Cancer Predisposition Screening Tool for Predicting Subsequent Malignant Neoplasms in Childhood Cancer Survivors. J Clin Oncol 39 (29): 3207-3216, 2021.
- Goudie C, Witkowski L, Cullinan N, et al.: Performance of the McGill Interactive Pediatric OncoGenetic Guidelines for Identifying Cancer Predisposition Syndromes. JAMA Oncol 7 (12): 1806-1814, 2021.
- Qin N, Wang Z, Liu Q, et al.: Pathogenic Germline Mutations in DNA Repair Genes in Combination With Cancer Treatment Exposures and Risk of Subsequent Neoplasms Among Long-Term Survivors of Childhood Cancer. J Clin Oncol 38 (24): 2728-2740, 2020.
- Collins A, Harrington V: Repair of oxidative DNA damage: assessing its contribution to cancer prevention. Mutagenesis 17 (6): 489-93, 2002.
- Gibson TM, Karyadi DM, Hartley SW, et al.: Polygenic risk scores, radiation treatment exposures and subsequent cancer risk in childhood cancer survivors. Nat Med 30 (3): 690-698, 2024.
- Im C, Sharafeldin N, Yuan Y, et al.: Polygenic Risk and Chemotherapy-Related Subsequent Malignancies in Childhood Cancer Survivors: A Childhood Cancer Survivor Study and St Jude Lifetime Cohort Study Report. J Clin Oncol 41 (27): 4381-4393, 2023.
- Landier W, Bhatia S, Eshelman DA, et al.: Development of risk-based guidelines for pediatric cancer survivors: the Children's Oncology Group Long-Term Follow-Up Guidelines from the Children's Oncology Group Late Effects Committee and Nursing Discipline. J Clin Oncol 22 (24): 4979-90, 2004.
- Kremer LC, Mulder RL, Oeffinger KC, et al.: A worldwide collaboration to harmonize guidelines for the long-term follow-up of childhood and young adult cancer survivors: a report from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Pediatr Blood Cancer 60 (4): 543-9, 2013.
- Mulder RL, Hudson MM, Bhatia S, et al.: Updated Breast Cancer Surveillance Recommendations for Female Survivors of Childhood, Adolescent, and Young Adult Cancer From the International Guideline Harmonization Group. J Clin Oncol 38 (35): 4194-4207, 2020.
- Kriege M, Brekelmans CT, Boetes C, et al.: Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med 351 (5): 427-37, 2004.
- Leach MO, Boggis CR, Dixon AK, et al.: Screening with magnetic resonance imaging and mammography of a UK population at high familial risk of breast cancer: a prospective multicentre cohort study (MARIBS). Lancet 365 (9473): 1769-78, 2005 May 21-27.
- Tieu MT, Cigsar C, Ahmed S, et al.: Breast cancer detection among young survivors of pediatric Hodgkin lymphoma with screening magnetic resonance imaging. Cancer 120 (16): 2507-13, 2014.
- Saslow D, Boetes C, Burke W, et al.: American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin 57 (2): 75-89, 2007 Mar-Apr.
- Berrington de Gonzalez A, Berg CD, Visvanathan K, et al.: Estimated risk of radiation-induced breast cancer from mammographic screening for young BRCA mutation carriers. J Natl Cancer Inst 101 (3): 205-9, 2009.
- Young KC, Burch A, Oduko JM: Radiation doses received in the UK Breast Screening Programme in 2001 and 2002. Br J Radiol 78 (927): 207-18, 2005.
- Spelic DC: Trends in Mammography Dose and Image Quality 1974-2005. Silver Spring, Md: U.S. Food and Drug Administration, 2006. Available online. Last accessed August 21, 2023.
- Clement SC, Kremer LCM, Verburg FA, et al.: Balancing the benefits and harms of thyroid cancer surveillance in survivors of Childhood, adolescent and young adult cancer: Recommendations from the international Late Effects of Childhood Cancer Guideline Harmonization Group in collaboration with the PanCareSurFup Consortium. Cancer Treat Rev 63: 28-39, 2018.
Late Effects of the Central Nervous System
Neurocognitive
Neurocognitive late effects are commonly observed after treatment of malignancies that require central nervous system (CNS)–directed therapies, including the following:
- Cranial radiation therapy.
- Systemic therapy with high-dose methotrexate or cytarabine.
- Intrathecal chemotherapy.
- Neurosurgical procedures.[1,2]
Children with CNS tumors or acute lymphoblastic leukemia (ALL) are most likely to be affected. Risk factors for the development of neurocognitive late effects include the following:[3,4,5,6,7]
- Female sex.
- Younger age at the time of treatment.
- Tumor location.
- Treatment with cranial radiation therapy and/or chemotherapeutic agents (systemic or intrathecal).
- Higher cranial radiation dose.
- Time since treatment.
Cognitive phenotypes observed in childhood survivors of ALL and CNS tumors may differ from traditional developmental disorders. For example, the phenotype of attention problems in ALL and brain tumor survivors appears to differ from developmental attention-deficit/hyperactivity disorder (ADHD) in that few survivors demonstrate significant hyperactivity/impulsivity, but instead have associated difficulties with processing speed and executive function.[8,9]
A Pediatric Normal Tissue Effects in the Clinic (PENTEC) comprehensive review was performed to develop models to facilitate the identification of dose constraints for radiation-associated CNS morbidities.[10]
- Models suggest a 5% risk of a subsequent intelligence quotient (IQ) lower than 85 when the following occurs:
- 10% of the brain is irradiated to 35.7 Gy.
- 20% of the brain is irradiated to 29.1 Gy.
- 50% of the brain is irradiated to 22.2 Gy.
- 100% of the brain is irradiated to 18.1 Gy.
- Note: All at 2 Gy/fraction and without methotrexate.
- Methotrexate exposure increased the risk of an IQ score lower than 85, similar to a generalized uniform brain radiation dose of 5.9 Gy. However, a limitation to this analysis was a lack of data about the total methotrexate doses, both intravenous and intrathecal.
- The model for predicting expected IQ, which also included the effect of dose, age, and methotrexate, suggested that each of these factors has an independent but probably cumulative effect on IQ.
In addition to the direct effects of neurotoxic therapies like cranial radiation, Childhood Cancer Survivor Study (CCSS) investigators observed that chronic health conditions resulting from non-neurotoxic treatment exposures (e.g., thoracic radiation) can adversely impact neurocognitive function presumably mediated by chronic cardiopulmonary and endocrine dysfunction.[11] In addition, some sequelae of neurotoxic therapy (e.g., severe hearing loss) have been associated with neurocognitive deficits independent of the neurotoxic treatment received.[12]
A related investigation from the CCSS evaluated longitudinal associations between physical activity and neurocognitive problems in adult survivors of childhood cancer.[13]
- Survivors were less likely than their siblings to report consistent physical activity (28.1% vs. 33.6%).
- Survivors who reported more consistent physical activity had fewer neurocognitive problems and larger improvements in cognitive concerns years after treatment.
- Body mass index (BMI) and severe chronic health conditions partially mediated the physical activity–neurocognitive associations, but the mediation effects were small.
A subsequent systematic review and meta-analysis compared the effects of physical activity or exercise interventions on cognitive function among individuals diagnosed with cancer (aged 0–19 years) with that of controls. Twenty-two unique studies (16 randomized controlled trials) were found with data on 12,767 individuals.[14] The median age at the start of the study was 12 years (interquartile range [IQR], 11–14 years), the median time from the end of cancer treatment was 2.5 years (IQR, 1.1–3.0 years), and the median intervention period was 12 weeks (IQR, 10–24 weeks).
- Compared with controls, there was moderate-quality evidence that physical activity and exercise improved cognitive performance measures and patient-reported measures of cognitive function in cancer survivors.
Childhood cancer survivors may be at risk for cognitive decline throughout their lives (even if not present in the first 10 years after therapy). In a study of 2,375 adult survivors of childhood ALL, Hodgkin lymphoma, or CNS tumors (mean age at evaluation, 31.8 years) and their sibling controls, new onset memory impairment emerged more often in survivors, decades after cancer diagnosis and treatment.[15]
- Compared with siblings, a higher proportion of survivors with no impairment in memory at baseline had new-onset memory impairment at follow-up, as follows:
- Sibling proportion, 7.8%.
- ALL survivors treated with chemotherapy only, 14.0%.
- ALL survivors treated with cranial radiation therapy, 25.8%.
- CNS tumor survivors, 34.7%.
- Hodgkin lymphoma survivors, 16.6%.
- Factors associated with new-onset memory impairment included cranial radiation in survivors of CNS tumor (relative risk [RR], 1.97) and dose of 8,000 mg/m2 or more of alkylator chemotherapy in survivors of ALL treated without cranial radiation therapy (RR, 2.80).
- Neurological conditions mediated the impact of cranial radiation therapy on new-onset memory impairment in survivors of CNS tumors.
- Smoking, obesity, low education attainment, and low physical activity were associated with an elevated risk of new onset-memory impairment.
Neurocognitive outcomes in brain tumor survivors
Long-term cognitive effects caused by illness and associated treatments are well-established morbidities in survivors of childhood and adolescent brain tumors. Risk factors for adverse neurocognitive effects in this group include the following:
- Cranial radiation therapy.
- Cranial radiation therapy has been associated with the highest risk of long-term cognitive morbidity, particularly in younger children.[3,4]
- There is an established dose-response relationship, with patients who receive higher-dose cranial radiation therapy consistently performing more poorly on intellectual measures.[3,4,16]
- Radiation dose to specific regions of the brain, including the temporal lobes and hippocampi, have been shown to significantly impact longitudinal IQ scores and academic achievement scores among children treated with craniospinal irradiation for medulloblastoma.[17]
- Tumor site.[3]
- Shunted hydrocephalus.[18,19]
- Postsurgical cerebellar mutism.[20]
- Auditory difficulties, including sensorineural hearing loss.[12,18]
- History of stroke.[21]
- Seizures.[3,22]
- Socioeconomic status (SES).[23]
The negative impact of radiation treatment has been characterized by changes in IQ scores, which have been noted to drop about 2 to 5 years after diagnosis.[24,25,26]
- The decline continues 5 to 10 years afterward, although less is known about potential stabilization or further decline of IQ scores several decades after diagnosis.[24,26]
- The decline in IQ scores over time typically reflects the child's failure to acquire new abilities or information at a rate similar to that of his or her peers, rather than a progressive loss of skills and knowledge.[27]
- Affected children also may experience deficits in other cognitive areas, including academic domains (reading and math) and problems with attention, processing speed, memory, and visual or perceptual motor skills.[28]
- Changes in cognitive functioning may be partially explained by radiation-induced reduction of normal-appearing white matter volume or integrity of white matter pathways, as evaluated through magnetic resonance imaging (MRI).[29,30]
- Reduced white matter integrity has been directly linked to slowed cognitive processing speed in survivors of brain tumors,[31] while greater white matter volume has been associated with better working memory, particularly in females.[30]
- Data from contemporary protocols show that using lower doses of cranial radiation, proton beam radiation, and more targeted treatment volumes appears to reduce the severity of neurocognitive effects of therapy.[3,19]
Evidence (predictors of cognitive decline among survivors of CNS tumors):
Longitudinal cohort studies have provided insight into the trajectory and predictors of cognitive decline among survivors of CNS tumors.
- A multisite, prospective, longitudinal trial evaluated predictors of cognitive performance among 139 infants with brain tumors who were treated with chemotherapy, with or without focal proton or photon radiation therapy.[32]
- IQ, parent-reported working memory, and parent-reported adaptive functioning were worse than normative expectations at baseline, with younger age and lower SES representing predictive factors.
- IQ remained stable over time, whereas parent-reported attention and executive dysfunction increased.
- Cognitive outcomes did not differ by treatment exposure (chemotherapy only vs. chemotherapy with radiation therapy).
- Changes in cognitive function were associated with supratentorial tumor location and cerebrospinal fluid diversion.
- St. Jude Children's Research Hospital (SJCRH) studied 78 children younger than 20 years (mean, 9.7 years) diagnosed with a low-grade glioma.[33]
- Cognitive decline after 54 Gy of conformal cranial radiation therapy was noted (see Figure 5).
- Age at time of cranial irradiation was more important than was cranial radiation dose in predicting cognitive decline, with children younger than 5 years estimated to experience the greatest cognitive decline.
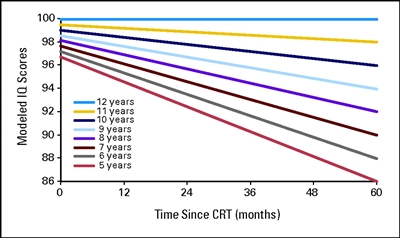
Figure 5. Modeled intelligence quotient (IQ) scores after conformal radiation therapy (CRT) by age for pediatric low-grade glioma. Age is measured in years, and time is measured in months after the start of CRT. Thomas E. Merchant, Heather M. Conklin, Shengjie Wu, Robert H. Lustig, and Xiaoping Xiong, Late Effects of Conformal Radiation Therapy for Pediatric Patients With Low-Grade Glioma: Prospective Evaluation of Cognitive, Endocrine, and Hearing Deficits, Journal of Clinical Oncology, volume 27, issue 22, pages 3691-3697. Reprinted with permission. © (2009) American Society of Clinical Oncology. All rights reserved.
- In a study of 51 children with low-grade gliomas and low-grade glioneural tumors diagnosed within the first year of life, the following was reported:[34]
- Mean IQ score was 75.5; 75% of the children had IQ scores lower than 85.
- Predictors of low IQ included a supratentorial location of the primary tumor and treatment with more chemotherapy regimens but not radiation use.
- The child's ability to complete age-appropriate tasks was as affected as IQ scores.
- A study of 126 medulloblastoma survivors treated with 23.4 Gy or 36 Gy to 39.6 Gy of craniospinal radiation (with a conformal boost dose of 55.8 Gy to the primary tumor bed) assessed processing speed, attention, and memory performance.[35]
- Processing speed scores declined significantly over time, while less decline was observed in attention and memory performance. Higher doses of radiation and younger age at diagnosis predicted slower processing speed over time.
- Studies of working memory and academic achievement in patients enrolled on the same medulloblastoma trial (SJCRH SJMB03 [NCT00085202]) indicated that performance was largely within the age-expected range up to 5 years postdiagnosis,[36,37] although in both studies, posterior fossa syndrome, higher cranial radiation dose, and younger age at diagnosis predicted worse performance over time.
- Serious hearing loss was associated with intellectual and academic decline over time.[37]
- In a prospective study of 178 children with medulloblastoma, 60 (34%) developed posterior fossa syndrome. Of these patients, 40 (23%) developed complete mutism and 20 (11%) developed diminished speech.[38]
- All children with posterior fossa syndrome had severe ataxia, and 42.5% of patients with posterior fossa syndrome and complete mutism had movement disorders.
- Independent risk factors for posterior fossa syndrome included younger age and surgery in a low-volume surgery center. Risk was lower among children with sonic hedgehog (SHH) tumors.
- Speech and gait returned in children with posterior fossa syndrome and complete mutism at a median of 2.3 and 0.7 months, respectively. Speech and gait returned in children with posterior fossa syndrome and diminished speech at a median of 2.1 and 1.5 months, respectively. However, with 12 months of follow-up, 12 of 27 children (44.4%) with posterior fossa syndrome and complete mutism were nonambulatory at 1 year.
- The presence of a movement disorder or high ataxia score was associated with delayed speech recovery, whereas older age and high ataxia score were associated with delayed gait return.
- Symptoms improved in all children, but no child with posterior fossa syndrome had a normal neurological examination at a median of 23 months after surgery.
- A prospective study compared 36 pediatric patients with medulloblastoma who experienced posterior fossa syndrome with 36 patients with medulloblastoma who did not experience posterior fossa syndrome but were matched on treatment and age at diagnosis.[38,39]
- The posterior fossa syndrome group demonstrated lower mean scores at 1, 3, and 5 years postdiagnosis on general intellectual ability, processing speed, working memory, and spatial relations compared with the non–posterior fossa syndrome group.
- The group who experienced posterior fossa syndrome showed little recovery over time and further decline over time in some domains (attention and working memory), compared with the non–posterior fossa syndrome group.
- Canadian investigators evaluated the impact of radiation (dose and boost volume) and neurological complications on patterns of intellectual functioning in a cohort of 113 medulloblastoma survivors (mean age at diagnosis, 7.5 years; mean time from diagnosis to last assessment, 6 years).[4]
- Survivors treated with reduced-dose craniospinal radiation therapy plus tumor bed boost showed stable intellectual functioning.
- Neurological complications, such as hydrocephalus requiring cerebrospinal fluid diversion and mutism, and treatment with higher doses and larger boost volumes of radiation resulted in intellectual declines with distinctive trajectories.
- Studies are beginning to examine cognitive outcomes in histologically distinct subtypes of brain tumors.
- Data from a sample of 121 medulloblastoma patients demonstrated variation in cognitive outcomes by four distinct molecular subgroups and differences in patterns of change over time.[40]
- Future research is required to establish if neurocognitive outcomes vary across biologically distinct subtypes of childhood brain tumors.
- SES has been shown to predict long-term cognitive outcomes in brain tumor survivors. In a prospective, longitudinal, phase II study of 248 children who were treated with conformal radiation therapy (54–59.4 Gy) for ependymoma, low-grade glioma, or craniopharyngioma, patients were monitored serially with cognitive assessment for 10 years.[23]
- At preradiation therapy baseline, significant associations were seen between SES and IQ, reading and math scores, sustained attention, and adaptive function. Higher SES was associated with better performance (P < .005).
- SES predicted change over time in IQ and reading and math scores. Higher SES was associated with less decline (P < .001).
- These results suggest that higher SES is a protective factor for cognitive late effects.
Evidence (predictors of cognitive decline among long-term survivors of CNS tumors):
Although adverse neurocognitive outcomes observed 5 to 10 years after treatment are presumed to be pervasive, and potentially worsen over time, few empirical data are available regarding the neurocognitive functioning in very long-term survivors of CNS tumors.
- A longitudinal study evaluated the relationship of hippocampal dose and short-term memory decline in 80 children and adolescents with low-grade gliomas (median age, 9.5 years at treatment) who received 54 Gy of radiation therapy.[41]
- At a median neurocognitive follow-up of 9.8 years, higher hippocampal dose (volume receiving 40 Gy) was associated with a greater decline in delayed recall.
- Among adult survivors participating in the CCSS, CNS tumor survivors (n = 802) self-reported significantly more problems with attention/processing speed, memory, emotional control, and organization than did survivors of non-CNS malignancies (n = 5,937) and sibling controls (n = 382).[42]
- Another CCSS study evaluating patterns of late mortality and morbidity in 2,821 adult survivors of CNS tumors reported impairment on measures of attention/processing speed (42.9%–73.3%) and memory (14.3%–37.4%), with differences observed by diagnosis and cranial radiation dose.[43]
- A study of 224 adult survivors of pediatric brain tumors participating in the St. Jude Life (SJLIFE) cohort study revealed that 20% to 30% of the survivors demonstrated severe neurocognitive impairment (defined as at least two standard deviations below normative mean) on clinical assessments of intelligence, memory, and executive function (e.g., planning, organization, and flexibility).[3]
- Among adults in the general population, the expected impairment rate at this threshold is 2%.
- Survivors who received whole-brain cranial irradiation were 1.5 to 3 times more likely to have severe neurocognitive impairment than were survivors who did not receive any cranial irradiation.
- Hydrocephalus with shunt placement and seizures were also associated with increased risk of impairment.
- In the CCSS, investigators compared long-term neuropsychological and SES outcomes of 181 adult survivors of pediatric low-grade gliomas with the outcomes of an age-matched and sex-matched sibling comparison group.[44]
- Survivors who were treated with surgery and radiation therapy (median age at diagnosis, 7 years; median age at assessment, 41 years) scored lower on estimated IQ than did survivors who were treated with surgery only, who scored lower than siblings (surgery and radiation therapy, 93.9; surgery only, 101.2; siblings, 108.5; all P values < .0001).
- Younger age at diagnosis was predictive of low scores for all neuropsychological outcomes except for attention/processing speed.
- Survivors who were treated with surgery and radiation therapy had more-than-twofold–lower occupation scores, income, and education than did survivors who were treated with surgery only.
- In a retrospective review of 528 brain tumor survivors diagnosed between 2000 and 2015, the prevalence of a clinical diagnosis of ADHD was 13.1%.[45]
- Of the survivors, 12.1% used medications for ADHD, and 19.9% of survivors had symptoms of ADHD without a clinical diagnosis.
- ADHD diagnosis was associated with younger age at tumor diagnosis and supratentorial tumor location, but not with sex, tumor type, or treatment type.
The neurocognitive consequences of CNS disease and treatment may have a considerable impact on functional outcomes for brain tumor survivors.
- In childhood and adolescence, neurocognitive deficits have been associated with poor social adjustment, including problems with peer relations, social withdrawal, and reduced social skills.[46,47]
- CNS tumor survivors are more likely to need special education services than are survivors of other malignancies.[48]
- Adult CNS tumor survivors are less likely to live independently, marry, and graduate from college than are survivors of other malignancies and siblings.[49]
Cognitive outcomes after proton radiation therapy
Data are emerging regarding cognitive outcomes after proton radiation to the CNS.[50,51,52] However, these studies have been limited by retrospective analysis of cognitive outcomes among relatively small clinically heterogenous pediatric brain tumor cohorts and the use of historically treated photon patients or population standards as comparison groups.
- In studies largely describing IQ changes during early follow-up (<5 years from radiation), results demonstrate lack of difference in slopes of IQ change among photon-treated and proton-treated patients [50] and significant declines in cognitive processing speed among patients treated with proton radiation.[51]
- One study compared the intellectual trajectories between pediatric patients with medulloblastoma who were treated with proton and photon radiation therapy (4.3-year mean follow-up after median 23.4-Gy craniospinal irradiation dose). Notably, boost dose and margins were significantly different between the two groups.[52]
- Children treated with proton radiation therapy exhibited superior long-term outcomes in global IQ, perceptual reasoning, and working memory compared with children who were treated with photon radiation therapy.
- The photon radiation therapy group exhibited a significant decline in global IQ, working memory, and processing speed.
- The proton radiation therapy group exhibited stable scores over time in all domains, except for processing speed.
Considering the relatively brief follow-up time from radiation, longitudinal follow-up is important to determine whether proton radiation provides a clinically meaningful benefit in sparing cognitive function compared with photon radiation. In addition, more targeted radiation treatment volumes with photons may diminish potential differences.
Neurocognitive outcomes in acute lymphoblastic leukemia (ALL) survivors
To minimize the risk of late cognitive sequelae, contemporary therapy for ALL uses a risk-stratified approach that reserves cranial irradiation for children who are considered at high risk of CNS relapse.
ALL and cranial radiation
In survivors of ALL, cranial radiation therapy may result in clinical and radiographic neurological late sequelae, including the following:
- Clinical leukoencephalopathy. Clinical leukoencephalopathy characterized by fluctuating encephalopathy, stroke-like symptoms, spasticity, ataxia, dysarthria, dysphagia, hemiparesis, and seizures is uncommon after contemporary ALL therapy. Neuroimaging frequently demonstrates white matter abnormalities among survivors treated with cranial irradiation and/or high-dose methotrexate.
- Radiographic leukoencephalopathy has been reported in up to 80% of children on some treatment regimens.
- Higher doses and more courses of intravenous methotrexate have been reported to increase risk of leukoencephalopathy.[53]
- In many patients, white matter anomalies are transient and decrease in prevalence, extent, and intensity with longer elapsed time from completion of therapy.[53]
- Leukoencephalopathy results in smaller white matter volumes that have been correlated with cognitive deficits.[53]
- Although these abnormalities are mild among the irradiated patients (overall IQ decline of approximately 10 points), those who have received higher doses at a young age may have significant learning difficulties.[54,55]
- Neurocognitive deficits. Deficits in neurocognitive functions such as visual-motor integration, processing speed, attention, and short-term memory are reported in children treated with 18 Gy to 24 Gy.[54,56,57]
- Females and children treated at a younger age are more vulnerable to the adverse impact of cranial radiation on the developing brain.[5]
- The decline in intellectual functioning appears to be progressive, showing more impairment of cognitive function with increasing time since radiation therapy.[5,6]
- Limited studies suggest that long-term survivors of childhood ALL treated with cranial irradiation are at risk of progressive decline consistent with early-onset mild cognitive impairment; this risk is most prominent among those treated with cranial radiation doses of 24 Gy.[58,59]
ALL and chemotherapy-only CNS therapy
Because of its penetrance into the CNS, systemic methotrexate has been used in a variety of low-dose and high-dose regimens for leukemia CNS prophylaxis.
- Systemic methotrexate in high doses with or without radiation therapy can lead to an infrequent but well-described leukoencephalopathy, which has been linked to neurocognitive impairment.[53]
- When neurocognitive outcomes after radiation therapy and chemotherapy-only regimens are directly compared, the evidence suggests a better outcome for those treated with chemotherapy alone, although some studies show no significant difference.[60,61]
- In a longitudinal analysis of 210 childhood ALL survivors, the development of acute leukoencephalopathy during chemotherapy-only CNS therapy predicted higher risks of developing long-term neurobehavioral problems (e.g., deficits in organization and task initiation [components of executive function]) and reduced white matter integrity in frontal brain regions.[62]
- Compared with cranial irradiation, chemotherapy-only CNS-directed treatment produces neurocognitive deficits involving processes of attention, speed of information processing, memory, verbal comprehension, visual-spatial skills, visual-motor functioning, and executive functioning. Global intellectual function is typically preserved.[56,60,63,64,65]
- Few longitudinal studies evaluating long-term neurocognitive outcome report adequate data for a decline in global IQ after treatment with chemotherapy alone.[63]
- The academic achievement of ALL survivors in the long term seems to be generally average for reading and spelling, with deficits mainly affecting arithmetic performance.[60,66]
- Risk factors for poor neurocognitive outcome after chemotherapy-only CNS-directed treatment are younger age and female sex.[65,67]
- Reduced cognitive status has been observed in association with reduced integrity in neuroanatomical regions essential in memory formation (e.g., reduced hippocampal volume with increased activation and thinner parietal cortices).[62]
- The long-term impact of these prevalent neurocognitive and neuroimaging abnormalities on functional status in aging adults treated for childhood ALL, particularly those treated with contemporary approaches using chemotherapy alone, remains an active area of research.
- Research in childhood ALL survivors treated with chemotherapy alone suggests that genetic predisposition may modulate risk of developing neurocognitive late effects. It also provides insights into potential mechanisms underlying neurocognitive deficits.[68,69]
Evidence (neurocognitive functioning in large pediatric cancer survivor cohorts):
- CCSS investigators identified sex-specific associations between treatment and chronic health conditions with neurocognitive impairment among 1,207 survivors of ALL (mean age, 30.6 years) who were treated with chemotherapy only.[7]
- Both male and female survivors reported increased prevalence of impaired task efficiency (attention and processing speed; adjusted odds ratio [OR], 1.89 for males; OR, 1.50 for females) and impaired memory (OR, 1.89 for males; OR, 1.96 for females) compared with 2,273 same-sex siblings.
- Among male survivors, impaired task efficiency was associated with grades 2 to 4 neurological conditions (OR, 4.33) and pulmonary conditions (OR, 4.99). Impaired memory was associated with increased cumulative dose of intrathecal methotrexate (OR, 1.68) and exposure to dexamethasone (OR, 2.44).
- In female survivors, grades 2 to 4 endocrine conditions were associated with higher risk of impaired task efficiency (OR, 2.19) and memory (OR, 2.26).
- The CCSS examined parent-reported cognitive, behavior, and learning problems from 1,560 adolescent survivors of childhood ALL who were treated with chemotherapy alone between 1970 and 1999.[70]
- Survivors treated with cranial irradiation had significantly higher frequency of problems in anxiety-depression, inattention-hyperactivity, and social withdrawal than did patients who were not treated with cranial irradiation.
- Compared with siblings, survivors treated with chemotherapy only were more likely to demonstrate headstrong behavior (19% of survivors vs. 14% of siblings, P = .010), inattention-hyperactivity (19% vs. 14%, P < .0001), social withdrawal (18% vs. 12%, P = .002), and had higher rates of learning problems (28% vs. 14%, P < .0001).
- In multivariable models among survivors, increased cumulative dose of intravenous methotrexate (i.e., >4.3 g/m2) conferred increased risk of inattention-hyperactivity (RR, 1.53).
- Adolescent survivors with cognitive or behavior problems and those with learning problems were less likely to graduate from college as young adults than adolescent survivors without cognitive or behavior problems.
- Inattention and hyperactivity problems were associated with the highest risk of special education placement during adolescence. Participation in special education during adolescence did not improve adult educational attainment.
- The SJCRH TOTAL XVI (NCT00549848) trial evaluated whether a higher dose of pegaspargase and early intensification of triple intrathecal therapy (ITT; methotrexate, hydrocortisone, and cytarabine) would improve systemic and CNS control in children with newly diagnosed ALL. Intensified ITT was defined as more than 21 cumulative doses for patients with low-risk ALL (70 of 194) and more than 27 doses for those with standard- and high-risk ALL (81 of 206). Neurocognitive testing was completed at the end of therapy.[71]
- The overall group had below age-based norms on measures of global intelligence (P < .0001), attention (P = .0051), working memory (P = .0001), processing speed (P = .0002), fine motor speed (P = .0001), and math skills (P = .0087). Caregiver ratings of patient functioning showed elevated risks of problems in attention (P = .0173), executive function (P = .0001), and adaptive skills (P = .0001).
- In the low-risk group, there were no significant differences between patients treated with and without intensified ITT.
- Patients with standard- and high-risk ALL who were treated with intensified ITT had poorer working memory (P = .0328) and fine motor speed (P = .0403), and elevated ratings of inattention (P = .0189) and executive dysfunction (P = .0245). Females in this risk group treated with intensified ITT had lower working memory scores.
- In the SJCRH Total XV (NCT00137111) trial, which omitted prophylactic cranial irradiation, comprehensive cognitive testing of 243 participants at week 120 revealed the following:[72]
- A higher risk of below-average performance on a measure of sustained attention but not on measures of intellectual functioning, academic skills, or memory.
- The risk of cognitive deficits correlated with treatment intensity but not with age at diagnosis or sex.
- Prolonged follow-up (average, 7.7 years from diagnosis) of this cohort demonstrated that intelligence was within normal limits compared with population expectations, but measures of executive function, processing speed, and memory were less than population means.
- Higher plasma methotrexate was associated with executive dysfunction, thicker cerebral cortex, and higher activity in frontal brain regions on functional MRI.
- In a large prospective study of neurocognitive outcomes in children with newly diagnosed ALL, 555 children were randomly assigned to receive CNS-directed therapy according to risk group.[73]
- The low-risk group was randomly assigned to receive either intrathecal methotrexate or high-dose methotrexate.
- The high-risk group was randomly assigned to receive either high-dose methotrexate or 24 Gy of cranial radiation therapy.
- A significant reduction in IQ scores (4–7 points) was observed in all patient groups when compared with controls, regardless of the CNS treatment delivered.
- Children younger than 5 years at diagnosis were more likely to have IQs below 80 at 3 years posttherapy than were children older than 5 years at diagnosis, irrespective of treatment allocation, suggesting that younger children are more vulnerable to treatment-related neurological toxic effects.
- Persistent cognitive deficits and progressive intellectual decline have been observed in cohorts of adults treated for ALL during childhood and associated with reduced educational attainment and unemployment.[5,55,59] The results of a study of more than 500 adult survivors of childhood ALL (average, 26 years postdiagnosis) showed the following:[55]
- Survivors demonstrated increased rates of impairment across all neurocognitive domains (ranging from 28.6%–58.9% for each domain).
- Rate of severe impairment increased as a function of cranial radiation dose and was common among survivors treated with lower doses of cranial irradiation and chemotherapy only.
- Impairment in executive function skills increased with time since diagnosis in a cranial radiation dose-dependent manner; impairment in intellect, academics, and memory progressively increased with younger age at treatment in a cranial radiation dose-dependent manner; and neurocognitive impairment was related to functional outcomes as adults, including reduced likelihood of college graduation and full-time employment.
ALL and steroid therapy
The type of steroid used for ALL systemic treatment may affect cognitive functioning.
- In a study that involved long-term neurocognitive testing (mean follow-up, 9.8 years) of 92 children with a history of standard-risk ALL who had received either dexamethasone or prednisone during treatment, no meaningful differences in mean neurocognitive and academic performance scores were observed.[74]
- In contrast, in a study of 567 adult survivors of childhood leukemia (mean age, 33 years; mean time since diagnosis, 26 years), the following was reported:[55]
- Dexamethasone exposure was associated with increased risk of impairment in attention (RR, 2.12; 95% confidence interval [CI], 1.11–4.03) and executive function (RR, 2.42; 95% CI, 1.20–4.91), independent of methotrexate exposure.
- Intrathecal hydrocortisone also increased risk of attention problems (RR, 1.24; 95% CI, 1.05–1.46).
Other cancers
Neurocognitive abnormalities have been reported in other groups of cancer survivors. A study of adult survivors of childhood non-CNS cancers (including ALL, n = 5,937) reported the following:[57]
- 13% to 21% of survivors reported impairment in task efficiency, organization, memory, or emotional regulation. This rate of impairment was approximately 50% higher than that reported in the sibling comparison group.
- Factors such as diagnosis before age 6 years, female sex, cranial radiation therapy, and hearing impediment were associated with impairment.
Emerging data suggest that the development of chronic health conditions in adulthood may contribute to cognitive deficits in long-term survivors of non-CNS cancers.
An SJLIFE cohort study evaluated whether children who experienced CNS injury were at higher risk of neurocognitive impairment associated with subsequent late-onset chronic health conditions. A total of 2,859 survivors who were aged 18 years or older and at least 10 years from diagnosis completed a neurocognitive battery and clinical examination. Of these patients, 1,598 had received CNS-directed therapy, including cranial radiation, intrathecal methotrexate, or neurosurgery.[75]
- CNS-treated survivors performed worse than non–CNS-treated survivors on all neurocognitive tests, and they were more likely to have global neurocognitive impairment (46.9% vs. 35.3%).
- A dose-response association was observed between severity/burden score of chronic health conditions and global neurocognitive impairment only among CNS-treated survivors (high OR, 2.24; 95% CI, 1.42–3.53; very high OR, 4.07; 95% CI, 2.30–7.17).
- Cardiovascular and pulmonary conditions were associated with cognitive outcomes (processing speed, executive function, and memory impairment) only in CNS-treated survivors with neurological conditions.
Neurocognitive abnormalities have been reported for the following cancers:
- Acute myeloid leukemia (AML). CCSS investigators compared the neurocognitive and psychosocial outcomes of 482 survivors (median age, 30 years) with those of 3,190 sibling controls (median age, 32 years).[76]
- Compared with siblings, AML survivors were more likely to report impairment in overall emotional (RR, 2.19; 95% CI, 1.51–3.18), neurocognitive (RR, 2.03; 95% CI, 1.47–2.79), and physical quality of life (RR, 2.71; 95% CI, 1.61–4.56) outcomes.
- Survivors were also at increased risk of psychosocial deficits, including lower educational attainment (RR, 1.15; 95% CI, 1.03–1.30), unemployment (RR, 1.41; 95% CI, 1.16–1.71), and lower income (RR, 1.39; 95% CI, 1.17–1.65).
- Outcomes were not statistically different between survivors who were treated with transplant and survivors who were treated with intensive chemotherapy alone.
- Osteosarcoma. In a study evaluating neurocognitive function among 80 long-term survivors of osteosarcoma (mean time since diagnosis, 24.7 years), survivors demonstrated lower mean scores in reading skills, attention, memory, and processing speed than did community controls.[77]
- The presence of cardiac, pulmonary, and endocrine conditions were significantly associated with worse performance on measures of memory and processing speed.
- Soft tissue sarcoma. A CCSS report characterized the prevalence of and risk factors for self-reported neurocognitive impairment in survivors of rhabdomyosarcoma (n = 713) and their siblings (n = 706). The report also identified risk factors associated with these outcomes in survivors.[78]
- Compared with their siblings, more survivors reported neurocognitive impairments (task efficiency: 21.1% vs. 13.7%; emotional regulation: 16.7% vs. 11.0%; memory: 19.3% vs. 15.1%). Cranial radiation exposure increased the risk of impaired task efficiency (OR, 2.30).
- Smoking was associated with impaired task efficiency (OR, 2.06) and memory (OR, 2.23).
- Neurological and hearing conditions were associated with impaired memory (OR, 2.44 and OR, 1.87, respectively).
SJLIFE study investigators evaluated neurocognitive function and health status through objective clinical assessments in 150 survivors of childhood soft tissue sarcoma (median age, 33 years; median time from diagnosis, 24 years).[79]
- Compared with community and population controls, survivors demonstrated lower measures of verbal reasoning, mathematics, and long-term memory.
- Cumulative anthracycline exposure (per 100 mg/m2) was found to be associated with poorer verbal reasoning, reading, and patient-reported vitality.
- Neurological and neurosensory chronic conditions were associated with poorer mathematics scores and hearing impairment.
- Better cognitive performance was associated with higher social attainment.
- Wilms tumor. SJLIFE study investigators examined the prevalence and predictors of neurocognitive outcomes, social attainment, emotional distress, and health-related quality of life in long-term survivors of pediatric Wilms tumor (n = 158; median time since diagnosis, 29 years; median age, 33 years) and compared the results to community controls.[80]
- Long-term Wilms tumor survivors demonstrated lower neurocognitive function, including verbal reasoning, academics, attention, memory, and executive function, than did controls.
- Wilms tumor survivors were less likely to graduate from college (OR, 2.23) and had more moderate-to-severe neurological conditions than did controls (18.4% vs. 8.2%; P < .001).
- Retinoblastoma. Serial assessment of cognitive and adaptive functioning in a group of retinoblastoma survivors younger than 6 years revealed declines in developmental functioning over time, with the most pronounced declines observed in patients with 13q deletions.[81]
- Further longitudinal follow-up of this cohort identified improvement in adaptive functioning in all treatment groups and in cognitive function in survivors who were treated with enucleation alone from the age of 5 years to the age of 10 years.[82]
- At age 10 years, overall functioning was generally within the average range, although estimated IQ was significantly below the normative mean for children who were treated with enucleation alone.[82]
A study of very long-term adult survivors, who were on average 33 years postdiagnosis, demonstrated largely average cognitive functioning across domains of intelligence, memory, attention, and executive function.[83]
- Lymphoma. Survivors of lymphoma have not historically been considered at risk of developing neurocognitive late effects.
- However, one report observed that more than two-thirds of survivors of childhood non-Hodgkin lymphoma experienced at least mild neurocognitive impairment, including severe deficits in executive function (13%), attention (9%), and memory (4%).[84]
- Similarly, in a study of 62 adult survivors of childhood Hodgkin lymphoma, survivors demonstrated worse performance on measures of sustained attention, short- and long-term memory, and cognitive fluency when compared with national normative data.[85] Importantly, measures of cardiac and pulmonary function were also associated with neurocognitive impairment in this group of survivors.
- Neuroblastoma. CCSS investigators compared cognitive outcomes among 837 survivors of neuroblastoma (median age, 1 year at diagnosis; median attained age, 25 years) and a sibling cohort (median attained age, 23 years) using the CCSS Neurocognitive Questionnaire (NCQ).[86]
- Survivors had a 50% higher risk of impairment with attention/processing speed and emotional regulation.
- The risk of neurocognitive impairments was higher among survivors with chronic health conditions.
- Survivors were also less likely to attain adult milestones, such as living independently.
Hematopoietic stem cell transplant (HSCT)
Cognitive and academic consequences of HSCT in children have also been evaluated and include, but are not limited to, the following:
- A survey study evaluated late neurocognitive outcomes among 199 survivors of HSCT (HSCT at age <21 years; median follow-up from HSCT, 27.6 years).[87]
- As assessed by the CCSS NCQ, 18.9% to 32.5% of survivors reported impairments in task efficiency, memory, emotional regulation, or organization, compared with the expected rate of 10% (general population).
- Quality of life, as assessed by Neuro-Quality of Life Cognitive Function Short Form (Neuro-QoL), among survivors (average T score, 49.6) was comparable to that of the normative population (50).
- Independent risk factors for impaired Neuro-QoL (T score <40) included hearing issues (OR, 4.7; 95% CI, 1.96–12.6), history of stroke or seizure (OR, 4.46; 95% CI, 1.44–13.8), and sleep disturbances (OR, 6.96; 95% CI, 2.53–19.1).
- SJCRH investigators examined the influence of age and conditioning with total-body irradiation (TBI) on the trajectory of cognitive function after HSCT. Among 315 patients who completed a baseline assessment, 183 were alive at 1 year after HSCT and completed additional assessments at 1, 3, and 5 years.[88]
- At 5 years after HSCT, younger patients (aged <3 years at baseline) who received TBI demonstrated a significantly lower IQ than those who did not receive TBI.
- Longitudinal analyses demonstrated a significant impact of age and TBI over time with declines in cognitive functioning during the first year among the youngest patients and recovery of functioning in subsequent years among patients who did not receive TBI.
- Young patients who received TBI failed to recover the losses experienced during the first year after HSCT, demonstrating stability in their functioning, but at a lower level.
Neurological Sequelae
Risk of neurological complications may be predisposed by the following:
- Tumor location.
- Neurosurgical procedures.
- Cranial radiation therapy.
- Spinal radiation therapy.
- Specific neurotoxic chemotherapeutic agents.
In children with CNS tumors, mass effect, tumor infiltration, and increased intracranial pressure may result in motor or sensory deficits, cerebellar dysfunction, and secondary effects such as seizures and cerebrovascular complications.[89]
Numerous reports describe abnormalities of CNS integrity and function, but such studies are typically limited by small sample size, cohort selection and participation bias, cross-sectional ascertainment of outcomes, and variable time of assessment from treatment exposures. In contrast, relatively few studies comprehensively or systematically ascertain outcomes related to peripheral nervous system function.
CNS tumor survivors remain at higher risk of new-onset adverse neurological events across their lifetimes than siblings. No plateau has been reached for new adverse sequelae, even 30 years from diagnosis, according to a longitudinal study of 1,876 5-year survivors of CNS tumors from the CCSS. The median time from diagnosis was 23 years, and the median age of the patients studied was 30.3 years.[90]
- Cranial radiation, stroke, tumor recurrence, and development of meningioma were independently associated with late-onset neurological sequelae (seizures, focal neurological dysfunction, and neurosensory abnormalities).
- This finding supports the need to monitor these patients carefully with continued neurological follow-up within or in close association with a multidisciplinary cancer survivor clinic.
Neurological complications that may occur in survivors of childhood cancer include the following:
Seizures
The development of seizures may occur secondary to tumor mass effect within the CNS and/or from neurotoxic CNS-directed therapies.
- In 1,876 5-year survivors of CNS tumors from the CCSS, the incidence of seizures increased from 27% in survivors 5 years from diagnosis to 41% in survivors 30 years from diagnosis.[90]
- Late-onset seizures were associated with frontal lobe radiation of 50 Gy (hazard ratio [HR], 1.8) and temporal lobe radiation in a dose-dependent fashion (HR, 1.9 for 1–49 Gy; HR, 2.2 for >50 Gy).
- Other risk factors associated with late-onset seizures included recurrence (HR, 2.3), development of meningioma (HR, 2.6), and history of stroke (HR, 2.0).
- The risk of seizures was elevated for survivors compared with siblings (HR, 12.7).
- Among survivors of childhood leukemia in the CCSS (N = 4,151; 64.5% treated with cranial irradiation), 6.1% reported the development of a seizure disorder, and seizures occurred more than 5 years after diagnosis in 51% of these patients.[91]
- An SJLIFE study evaluated the impact of seizure-related factors on neurocognitive, health-related quality of life (HRQOL), and social outcomes in 2,022 childhood cancer survivors (median age, 31.5 years; median time from diagnosis, 23.6 years).[92]
- Seizures were identified in 232 survivors (11.5%; 29.9% of survivors with CNS tumors and 9.0% of survivors without CNS tumors).
- Among CNS tumor survivors, seizures were associated with poorer (based on expected age-adjusted standard z-scores) executive function and processing speed. Seizure resolution was associated with improved attention and memory.
- Among non-CNS tumor survivors, seizures were associated with worse function in all cognitive domains compared with survivors without seizures. Seizure severity was associated with worse processing speed, and resolution of seizures was associated with better executive function and attention.
- Non-CNS survivors with seizures had poorer HRQOL outcomes (physical functioning, physical role limitations, and general health). Seizures in both non-CNS and CNS tumor survivors increased the risk of unemployment and part-time employment.
Peripheral neuropathy
Vinca alkaloid agents (vincristine and vinblastine) and heavy metals (cisplatin and carboplatin) may cause peripheral neuropathy.[93,94,95]
- Peripheral neuropathy presents during treatment and appears to improve or clinically resolve after completion of therapy.[93] However, recent studies of long-term survivors suggest that chemotherapy-induced peripheral neuropathy is likely under-ascertained.[96]
- Higher cumulative doses of vincristine and/or intrathecal methotrexate have been linked to neuromuscular impairments in long-term survivors of childhood ALL, which suggests that persistent effects of these agents may affect functional status in aging survivors.[93]
- SJLIFE study investigators observed associations between peripheral neuropathy and impairment in performance measures of movement (mobility and walking endurance) and quality of life (physical functioning, role physical, and general health) among survivors of childhood ALL.[97]
- Static-standing balance impairment (a predictor of falling within the next 90 days) was more common in survivors compared with controls but was not associated with peripheral neuropathy.[97]
- Among adult survivors of extracranial solid tumors of childhood (median time from diagnosis, 25 years), standardized assessment of neuromuscular function disclosed motor impairment in association with vincristine exposure and sensory impairment in association with cisplatin exposure.[94]
- Survivors with sensory impairment demonstrated a higher prevalence of functional performance limitations related to poor endurance and mobility restrictions.
Stroke or other cerebrovascular effects
- Childhood CNS tumor survivors have a 43-fold elevated risk of stroke compared with siblings.[43,98]
- Cranial radiation therapy (dose dependent), baseline atherosclerosis, hypertension, and African American ethnicity are identified risk factors.[99,100,101] For information about stroke, see the Cerebrovascular disease section.
- A British CCSS (n = 13,457 survivors) that included 2,885 childhood CNS tumor survivors reported the following:[102]
- CNS tumor survivors who were treated with cranial irradiation had an increased risk of developing cerebrovascular disease between the ages of 50 years and 65 years.
- Compared with an expected incidence of 4.2%, the cumulative incidence of cerebrovascular disease in survivors was 11.6% by age 40 years, 16% by age 50 years, and 26% by age 65 years.
- Among 271 CCSS participants with a history of stroke at a median age of 19 years, 70 reported a second stroke at a median age of 32 years.[103]
- The 10-year cumulative incidence of late recurrent stroke was 21% overall, and 33% for those treated with 50 Gy or higher cranial radiation therapy.
- Risk factors for recurrent stroke included the following:
- Cranial radiation therapy 50 Gy or higher (HR, 4.4; 95% CI, 1.4–13.7).
- Hypertension (HR, 1.9; 95% CI, 1.0–3.5).
- Older age at first stroke (HR, 6.4; 95% CI, 1.8–23).
- A PENTEC review identified 101 of 3,989 pediatric patients who experienced at least one cerebrovascular toxicity (transient ischemic attack, stroke, moyamoya, or arteriopathy).[104]
- Predicted incidences were based on the radiation dose to the Circle of Willis: 0.2% at 30 Gy, 1.3% at 45 Gy, and 4.4% at 54 Gy.
- At an attained age of 35 years, the predicted stroke incidence was 0.9% to 1.3% for 30 Gy, 1.8% to 2.7% for 45 Gy, and 2.8% to 4.1% for 54 Gy (compared with a baseline risk of 0.2%–1.0%).
- At an attained age of 45 years, the predicted stroke incidence was 1.2% to 4.2% for 30 Gy, 4.5% to 8.6% for 45 Gy, and 6.7% to 13% for 54 Gy (compared with a baseline risk of 0.5%–1.0%).
Hypersomnia (daytime sleepiness) or narcolepsy
- In a retrospective review of brain tumor patients treated at SJCRH, investigators identified 39 of 2,336 patients who were diagnosed with hypersomnia/narcolepsy, for a prevalence rate of 1,670 cases per 100,000, which is much higher than a prevalence rate of 20 to 50 cases per 100,000 reported in the general population.[105]
- This may be an underestimate in childhood brain tumor survivors because many patients with mild-to-moderate symptoms, such as fatigue and sleep disturbances, may not be recognized or referred to a sleep specialist.
- Hypersomnia/narcolepsy was diagnosed at a median of 6 years (range, 0.4–13.2 years) from tumor diagnosis and 4.7 years (range, 1.5–10.4 years) from cranial radiation.
- Midline tumor location and antiepilepsy drug use correlated with hypersomnia/narcolepsy, while radiation dose higher than 30 Gy trended toward significance.
- Posterior fossa tumor location was associated with a reduced risk of hypersomnia.
- Treatment of hypersomnia/narcolepsy should be individualized and pharmacologic intervention with stimulants may be beneficial.
- In a baseline evaluation of 82 childhood CNS tumor survivors (median age, 13.8 years) participating in a randomized controlled trial of neurofeedback, 48% of survivors endorsed sleep problems and scored significantly worse than the norm on the Sleep Disturbance Scale for Children in the subscales for initiating and maintaining sleep, excessive somnolence, and total scale.[106]
- Emotional problems and/or hyperactivity/inattention were independent potential risk factors for sleep problems. Sleep problems were also associated with worse parent-reported executive functioning.
Other neurological sequelae
- In a report from the CCSS that compared self-reported neurological late effects among 4,151 adult survivors of childhood ALL with siblings, survivors were at elevated risk for late-onset coordination problems, motor problems, seizures, and headaches.[91]
- The overall cumulative incidence was 44% at 20 years. Serious headaches were most common, with a cumulative incidence of 25.8% at 20 years, followed by focal neurological dysfunction (21.2%) and seizures (7%).
- Children who were treated with regimens that included cranial irradiation for ALL and those who suffered relapse were at increased risk for late-onset neurological sequelae.
- A cross-sectional study evaluated neurological morbidity and quality of life in 162 survivors of childhood ALL (median age at evaluation, 15.7 years; median time from completion of therapy, 7.4 years) in concert with a clinical neurological examination.[107]
- Neurological symptoms were present in 83% of survivors, but symptom-related morbidity was low and quality of life was high in most survivors.
- The most commonly reported symptoms included neuropathy (63%), headache (46.9%), dizziness (33.3%), and back pain (22.8%).
- Female sex, ten doses or more of intrathecal chemotherapy, cranial irradiation, CNS leukemia at diagnosis, and history of ALL relapse were associated with neurological morbidity.
- Neuroimaging studies of irradiated and nonirradiated ALL survivors demonstrate a variety of CNS abnormalities, including leukoencephalopathy, cerebral lacunes, cerebral atrophy, and dystrophic calcifications (mineralizing microangiopathy).[53,59,108,109]
- Among these, abnormalities of cerebral white matter integrity and volume have been correlated with neurocognitive outcomes.
- Cavernomas have also been observed in ALL survivors treated with cranial irradiation. They have been speculated to result from angiogenic processes as opposed to tumorigenesis.[110]
- In a retrospective cross-sectional study, 101 survivors of childhood ALL (mean time since diagnosis, 27.6 years) who were treated with cranial irradiation (63.4% received ≤18 Gy) underwent neurocognitive testing and 3T brain MRI.[111]
- Small focal intracerebral hemorrhages that are only visible on exquisitely sensitive MRI sequences were identified and localized using susceptibility weighted imaging.
- At least one microbleed was present in 85% of survivors, and they occurred more frequently in frontal lobes.
- A radiation dose of 24 Gy conveyed a fivefold greater risk of having multiple microbleeds when compared with a dose of 18 Gy.
- No significant difference was found in neurocognitive scores with either the absence or presence of microbleeds or their location.
- CCSS investigators evaluated treatment-related neurological sequelae in survivors of childhood CNS tumors.[90]
- In 1,876 5-year survivors of CNS tumors from the CCSS, the cumulative incidence of headaches increased from 38% at 5 years to 53% at 30 years since diagnosis.
- Coordination problems increased from 21% at 5 years to 53% at 30 years since diagnosis, and motor impairment increased from 21% to 35% during this same time period.
- Increased risk of motor impairment was associated with tumor recurrence (HR, 2.6), development of a meningioma (HR, 2.3), and stroke (HR, 14.9).
- The cumulative incidence of hearing loss increased from 9% at 5 years to 23% at 30 years, cumulative incidence of tinnitus increased from 8% at 5 years to 21% at 30 years, and cumulative incidence of vertigo increased from 9% at 5 years to 17% at 30 years.
- Risks of motor impairment (HR, 7.6) and hearing loss (HR, 18.4) were elevated compared with siblings.
- CCSS investigators estimated the prevalence and cumulative incidence of neuromuscular dysfunction (motor or sensory dysfunction) among 25,583 childhood cancer survivors and 5,044 siblings.[112]
- Neuromuscular dysfunction was prevalent in 14.7% of survivors 5 years after diagnosis, compared with 1.5% in siblings (prevalence ratio [PR], 9.9%; 95% CI, 7.9–12.4).
- The prevalence of neuromuscular dysfunction was highest in survivors of CNS tumors (PR, 27.6; 95% CI, 22.1–34.6) and sarcomas (PR, 11.5; 95% CI, 9.1–14.5).
- The 20-year cumulative incidence increased to 24.3% in survivors 20 years after diagnosis.
- Cancer treatments associated with increased prevalence of neuromuscular dysfunction included spinal radiation therapy, increasing doses of cranial radiation therapy, and platinum agents.
- Neuromuscular dysfunction was associated with downstream adverse outcomes, including concurrent or later obesity (PR, 1.1; 95% CI, 1.1–1.2), anxiety (PR, 2.5; 95% CI, 2.2–2.9), depression (PR, 2.1; 95% CI, 1.9–2.3), and lower likelihood of graduating college (PR, 0.92; 95% CI, 0.90–0.94) and finding employment (PR, 0.8; 95% CI, 0.8–0.9).
- SJLIFE investigators assessed motor and sensory impairment in 378 survivors of childhood CNS tumors (5 years or longer from diagnosis) and 445 age-, sex-, and race-matched controls, using the modified Total Neuropathy Score.[113]
- Among survivors, 91 (24.1%; 95% CI, 19.8%–29.4%) had any grade 2 or higher motor or sensory impairment (motor only, 27 [7.1%]; sensory only, 40 [10.6%]; both, 24 [6.4%]).
- Survivors were more likely than controls to have grade 2 or higher impairment (13.5% for survivors [7.7% for grade 2 and 5.8% for grade 3] vs. 0.9% for controls; P < .001).
- Survivors of ependymoma had the highest prevalence of motor impairment (22.0%), and survivors of medulloblastoma had the highest prevalence of sensory impairment (33.3%).
- Treatment factors associated with grade 2 or higher motor impairment in multivariable models included vinca alkaloid exposure of 15 mg/m2 or less compared with no exposure (OR, 4.38; 95% CI, 1.06–18.08) and etoposide exposure of more than 2,036 mg/m2 compared with no exposure (OR, 12.61; 95% CI, 2.19–72.72).
- Radiation myelopathy is a rare but severe complication of radiation therapy exposure. The PENTEC spinal cord task force examined the factors that potentially contribute to radiation myelitis in the pediatric population.[114]
- Thirty-two patients (treated between 1962 and 2002) with radiation myelopathy were identified, for a crude incidence of 0.5%. The median age was 13 years, and 52% of the patients were male. No apparent association was identified for age at the time of radiation therapy. The most common cancer diagnoses were rhabdomyosarcoma, medulloblastoma, and Hodgkin lymphoma.
- The median radiation dose was 40 Gy, and the fraction size was 1.8 Gy. The median latency period from completion of radiation therapy to development of radiation myelopathy was 7 months (range, 1–29 months), with higher radiation therapy doses correlating with longer latency periods (P = .03).
- The most common chemotherapies given to patients with radiation myelopathy were vincristine, intrathecal (IT) methotrexate, and IT cytarabine. Ten patients received vincristine, IT methotrexate, and IT cytarabine.
- Chemotherapy appears to reduce spinal cord tolerance to radiation. The radiation therapy dose resulting in radiation myelopathy was lower in patients who received chemotherapy than in those who did not receive chemotherapy (39.6 ± 8.7 Gy vs. 49.7 ± 8.2 Gy; P = .04).
- Eight of the 32 cases of radiation myelopathy occurred in patients treated on a single Intergroup Rhabdomyosarcoma Study Group (treated with intensive IT methotrexate and cytarabine chemotherapy).
- Many of the reports were from an era before CT-based treatment planning. Also, the investigators could not find any signs that the developing spinal cord is more sensitive than the adult spinal cord.
Table 4 summarizes CNS late effects and the related health screenings.
| Predisposing Therapy | Neurological Effects | Health Screening |
|---|---|---|
| IQ = intelligence quotient; IT = intrathecal; IV = intravenous. | ||
| a Adapted from theChildren's Oncology Group Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers. | ||
| Heavy metals (carboplatin, cisplatin) | Peripheral sensory neuropathy | Neurological examination |
| Vinca alkaloid agents (vinblastine, vincristine) | Peripheral sensory or motor neuropathy (areflexia, weakness, foot drop, paresthesias) | Neurological examination |
| Methotrexate (high dose IV or IT); cytarabine (high dose IV or IT); radiation exposing the brain | Clinical leukoencephalopathy (spasticity, ataxia, dysarthria, dysphagia, hemiparesis, seizures); headaches; seizures; sensory deficits | History: cognitive, motor, and/or sensory deficits, seizures |
| Neurological examination | ||
| Radiation exposing cerebrovascular structures | Cerebrovascular complications (stroke, Moyamoya disease, occlusive cerebral vasculopathy) | History: transient/permanent neurological events |
| Blood pressure test | ||
| Neurological examination | ||
| Neurosurgery–brain | Motor and/or sensory deficits (paralysis, movement disorders, ataxia, eye problems [ocular nerve palsy, gaze paresis, nystagmus, papilledema, optic atrophy]); seizures | Neurological examination |
| Neurology evaluation | ||
| Neurosurgery–brain | Hydrocephalus; shunt malfunction | Abdominal x-ray |
| Neurosurgery evaluation | ||
| Neurosurgery–spine | Neurogenic bladder; urinary incontinence | History: hematuria, urinary urgency/frequency, urinary incontinence/retention, dysuria, nocturia, abnormal urinary stream |
| Neurosurgery–spine | Neurogenic bowel; fecal incontinence | History: chronic constipation, fecal soiling |
| Rectal examination | ||
| Predisposing Therapy | Neurocognitive Effects | Health Screening |
| Methotrexate (high-dose IV or IT); cytarabine (high-dose IV or IT); radiation exposing the brain; neurosurgery–brain | Neurocognitive deficits (executive function, memory, attention, processing speed, etc.); learning deficits; diminished IQ; behavioral change | Assessment of educational and vocational progress |
| Formal neuropsychological evaluation | ||
Psychosocial
Many childhood cancer survivors report reduced quality of life, impaired health status, or other adverse psychosocial outcomes, compared with siblings or noncancer population groups.[115,116] Vulnerable groups have been identified related to sociodemographic factors (e.g., female sex), specific cancer diagnoses (e.g., CNS tumor), cancer treatments (e.g., cranial radiation therapy), health behaviors (e.g., smoking), and type/cumulative burden of chronic health conditions. The diagnosis of childhood cancer may also affect psychosocial outcomes and the expected attainment of functional and social independence in adulthood. Several investigations have demonstrated that survivors of pediatric CNS tumors are particularly vulnerable.[49,117]
Evidence for adverse psychosocial adjustment after childhood cancer has been derived from sources, ranging from patient-reported or proxy-reported outcomes to data from population-based registries. The former may be limited by small sample size, cohort selection and participation bias, and variable methods and venues (clinical vs. distance-based survey) of assessments. The latter is often not well correlated with clinical and treatment characteristics that permit the identification of survivors at high risk of psychosocial deficits.
Achievement of social milestones
Survivors with neurocognitive deficits are particularly vulnerable to deficits in achievement of expected social outcomes during adulthood.
- Adult survivors of childhood cancer participating in the CCSS who were treated with CNS-directed therapies did not achieve independence at rates comparable with survivors who did not receive CNS-directed therapies or their sibling counterparts. Associations between neurological late effects and attainment of independence were examined in adult survivors of cancer treated with (n = 7,881) and without CNS-directed therapies (n = 8,039) and a sibling cohort (n = 3,994). Compared with the other groups, survivors of childhood cancer treated with CNS-directed therapies showed three distinct patterns of functional independence: (1) moderately independent, never married, and nonindependent living (78.7%); (2) moderately independent, unable to drive (15.6%); (3) not independent (5.7%). No survivors treated with CNS-directed therapies were fully independent (a fourth identified class). In contrast, 50% of survivors who did not receive CNS treatment and 60% of siblings were classified as fully independent. Nonindependence was associated with emotional distress symptoms (i.e., depression, anxiety, somatization, and suicidal ideation).[118]
- In a population-based study of adult survivors of CNS tumors diagnosed in childhood or adolescence, survivors had significantly poorer self-perception and self-esteem than did individuals in the general population. Female sex, persistent visible physical sequelae, specific tumor type, and treatment with cranial radiation therapy predicted poor self-perception outcomes.[119]
- In a series of CNS malignancy survivors (n = 802) reported from the CCSS, adverse outcome on multiple indicators of successful adult adjustment (educational achievement, income, employment, and marital status) were most prevalent among survivors who reported neurocognitive dysfunction.[42]
- Collectively, studies evaluating psychosocial outcomes among CNS tumor survivors indicate deficits in social competence that worsen over time.[120] This includes problems with peer rejection and isolation in childhood/adolescence, and the inability to develop friendships and romantic relationships as adults.
- In an SJLIFE study of 224 survivors of CNS tumors (median current age, 26 years; median time from diagnosis, 18 years), neurocognitive impairment was significantly associated with lower educational attainment, unemployment, and dependent living.[3]
- Among one subgroup, significant impairments in social perceptions skills, including affect recognition, contributed to limited achievement of functional outcomes. Self-reports of social adjustment were generally within normal limits, suggesting limited self-insight into social deficits.[121]
- In a series of 1,560 adolescent survivors of childhood ALL treated with chemotherapy alone, the CCSS identified a significant proportion of survivors who still experienced problems with headstrong behavior, inattention-hyperactivity, and social withdrawal, which were associated with an increased risk of special education placement and predicted reduced adult educational attainment.[70]
- In a cross-sectional study of 855 childhood leukemia survivors (mean, 10.2 years from diagnosis) in the Leucémie de l'Enfant et de l'Adolescent (LEA) cohort, investigators identified independent factors associated with repeating a grade in school, including low parental education and household financial difficulties, emphasizing the importance of considering socioeconomic factors that may affect access to educational support. Survivors who were adolescents (aged 11–17 years) at diagnosis were also at greater risk than were survivors who were children (aged <11 years) at diagnosis.[122]
- In a population-based, cross-sectional, survivorship study, 28% of adolescent and young adult (AYA) survivors of sarcoma (aged 18–39 years at diagnosis; median time from diagnosis, 6.2 years) experienced impaired social functioning.[123] Multivariable analysis identified independent associations with impaired social functioning and unemployment (OR, 3.72; 95% CI, 1.26–10.97) and having to make lifestyle changes because of financial problems caused by an individual's physical condition or medical treatment (OR, 3.39; 95% CI, 1.12–10.30). In contrast, better social support reduced the risk of impaired social functioning (OR, 0.74; 95% CI, 0.57–0.96).
Psychological distress and suicidality
Childhood cancer survivors are also at risk of developing symptoms of psychological distress and suicidality.[124]
- A CCSS report characterized the prevalence of and risk factors for self-reported emotional distress and HRQOL in survivors of rhabdomyosarcoma (n = 713) and their siblings (n = 706). The study also identified risk factors associated with these outcomes in survivors.[78]
- Compared with their siblings, more survivors reported elevated emotional distress (somatic distress: 12.9% vs. 4.7%; anxiety: 11.7% vs. 5.9%; depression: 22.8% vs. 16.9%) and poorer HRQOL (physical functioning: 11.1% vs. 2.8%; role functioning due to physical problems: 16.8% vs. 8.2%; pain: 17.5% vs. 10.0%; vitality: 22.3% vs. 13.8%; social functioning: 14.4% vs. 6.8%; emotional functioning: 17.1% vs. 10.6%).
- Chest and pelvic radiation exposure predicted an increased risk of impaired physical functioning (OR, 2.68 and 3.44, respectively).
- Smoking was associated with anxiety (OR, 2.71) and depression (OR, 1.77).
- Neurological conditions increased the risk of anxiety (OR, 2.30), and hearing conditions increased the risk of depression (OR, 1.79).
- The SJLIFE study was used to compare the risks of suicidal ideation, suicidal behaviors, and mortality in adult survivors of childhood cancer with those of the general population.[125]
- Survivors (n = 3,096) reported a similar 12-month prevalence of suicidal ideation compared with the general population (standardized incidence ratio [SIR], 0.68) and a lower prevalence of suicidal behaviors (planning: SIR, 0.17; attempts: SIR, 0.07) and mortality (standardized mortality ratio, 0.60).
- Among survivors, depression (RR, 12.30), anxiety (RR, 2.19), and financial stress (RR, 1.47) were found to be risk factors associated with suicidal ideation.
- Survivors who were currently single, widowed, or divorced; who were not working full time; who reported financial stress during the previous year; and who reported sleep disturbances had an approximately 30% to 50% higher prevalence of suicidal ideation.
- A CCSS study evaluated the prevalence of recurrent suicidal ideation among 9,128 adult long-term survivors of childhood cancer.[126]
- Survivors were more likely to report late suicidal ideation (OR, 1.9; 95% CI, 1.5–2.5) and recurrent suicidal ideation (OR, 2.6; 95% CI, 1.8–3.8) compared with siblings.
- History of seizure was associated with a twofold increased likelihood of suicide ideation in survivors.
- A population-based study evaluated suicide among adults treated for cancer before age 25 years.[127]
- The absolute risk of suicide was low (24 cases among 3,375 deaths).
- The HR of suicide was increased among individuals treated for cancer in childhood (0–14 years; HR, 2.5; 95% CI, 1.7–3.8) and in adolescence and young adulthood (15–24 years; HR, 2.3; 95% CI, 1.2–4.6).
The presence of chronic health conditions can also impact aspects of psychological health.
- In a study that evaluated psychological outcomes among long-term survivors treated with HSCT, 22% of survivors and 8% of sibling controls reported adverse outcomes. Somatic distress was the most prevalent condition and affected 15% of HSCT survivors, representing a threefold higher risk compared with siblings. HSCT survivors with severe or life-threatening health conditions and active chronic GVHD had a twofold increased risk of somatic distress.[128]
- A report from the CCSS revealed that the presence of chronic pulmonary, endocrine, and cardiac conditions was associated with increased risk of psychological distress symptoms in a sample of 5,021 adult survivors of childhood cancer.[129]
- In a CCSS investigation that evaluated long-term psychological and educational outcomes among survivors of neuroblastoma, survivors demonstrated elevated risks of psychological impairment, which was associated with the use of special education services and lower educational attainment. The presence of two or more chronic health conditions, but not common treatment exposures, predicted psychological impairment. Specifically, pulmonary disease predicted impairment in all five psychological domains, whereas endocrine disease and peripheral neuropathy each predicted impairment in three domains.[130]
Incorporation of psychological screening into clinical visits for childhood cancer survivors may be valuable. However, limiting such evaluations to those returning to long-term follow-up clinics may result in a biased subsample of survivors with more difficulties, and precise prevalence rates may be difficult to establish.
- In a study of 101 adult survivors of childhood cancer, psychological screening was performed during a routine annual evaluation at the survivorship clinic at the Dana Farber Cancer Institute.[131]
- On the Symptom Checklist 90 Revised, 32 survivors had a positive screen (indicating psychological distress), and 14 survivors reported at least one suicidal symptom.
- Risk factors for psychological distress included survivors' dissatisfaction with physical appearance, poor physical health, and treatment with cranial irradiation.
- This instrument was shown to be feasible for use in the clinic-visit setting because the psychological screening was completed in less than 30 minutes and did not appear to cause distress in the survivors in 80% of cases.
For more information about psychological distress, depression, and cancer patients, see Adjustment to Cancer: Anxiety and Distress and Depression.
Serious mental illnesses
A population-based study from Taiwan compared the prevalence of serious mental illnesses in 5,121 childhood and adolescent cancer survivors with that of population controls.[132]
- Survivors (mean age, 9 years; 60% were 5 or more years from diagnosis) showed increased risks of six serious mental illnesses compared with controls. These disorders included the following:
- Autism spectrum disorder (HR, 10.42; 95% CI, 4.58–23.69).
- ADHD (HR, 6.59; 95% CI, 4.91–8.86).
- Bipolar disorder (HR, 2.93; 95% CI, 1.26–6.80).
- Major depressive disorder (HR, 1.88; 95% CI, 1.26–2.79).
- Obsessive-compulsive disorder (OCD) (HR, 3.37; 95% CI, 1.33–8.52).
- Post-traumatic stress disorder (PTSD) (HR, 6.10; 95% CI, 1.46–25.54).
- Survivors were younger than controls at the time of diagnosis of ADHD, schizophrenia, major depressive disorder, and OCD.
- Risks of serious mental illnesses varied according to specific cancer types. The greatest number of major psychiatric disorders was observed among survivors of brain cancer and lymphatic/hematopoietic tissue cancer.
A population-based study linked individuals with a history of six common cancers diagnosed at age 15 to 21 years to provincial health care data to compare rates of outpatient (family physician and psychiatrist) visits for psychiatric indications and time to severe psychiatric events (emergency room visit, hospitalization, and suicide). The study included 2,208 AYA cancer patients and 10,457 matched controls.[133]
- Five-year AYA survivors experienced higher rates of outpatient mental health visits than did controls (671 vs. 506 visits per 1,000 person-years; RR, 1.3), higher risk of a severe psychiatric episode (HR, 1.2), and higher risk of a psychotic disorder–associated severe event (HR, 2.0).
- Treatment in an adult center was associated with substantially higher outpatient visit rates compared with treatment in pediatric settings (RR, 1.8).
PTSD after childhood cancer
Despite the many stresses associated with the diagnosis of cancer and its treatment, studies have generally shown low levels of post-traumatic stress symptoms and PTSD in children with cancer, typically no higher than those in healthy comparison children.[134]
- The prevalence of PTSD and post-traumatic stress symptoms has been reported in 15% to 20% of young adult survivors of childhood cancer, with estimates varying based on criteria used to define these conditions.[135]
- In a cohort of 5,121 childhood and adolescent cancer survivors (mean age, 9 years), the incidence of PTSD was 0.59%. Compared with controls, survivors showed a 6.10-fold elevated risk of being diagnosed with PTSD. Brain cancer survivors had the highest risk of all cancer diagnoses for PTSD (HR, 18.50; 95% CI, 2.11–162.64).[132]
- Patient and parent adaptive style appear to be significant determinants of PTSD in the pediatric oncology setting.[136,137]
- Survivors with PTSD reported more psychological problems and negative beliefs about their illness and health status than did those without PTSD.[138,139]
- A subset of adult survivors (9%) from the CCSS reported functional impairment and/or clinical distress in addition to the set of symptoms consistent with a full diagnosis of PTSD.[140]
- PTSD was significantly more prevalent in survivors than in sibling comparisons.
- PTSD was significantly associated with being unmarried, having an annual income of less than $20,000, being unemployed, having a high school education or less, and being older than 30 years.
- Survivors who were treated with cranial irradiation before age 4 years were at particularly higher risk of developing PTSD.
- Intensive cancer-directed therapy was also associated with increased risk of full PTSD.
- Because avoidance of places and persons associated with the cancer is part of PTSD, the syndrome may interfere with obtaining appropriate health care.[141]
- Those with PTSD perceive greater current threats to their lives or the lives of their children.
- Other risk factors for PTSD include poor family functioning, decreased social support, and noncancer stressors.
Psychosocial outcomes among childhood, adolescent, and young adult cancer survivors
Most research on late effects after cancer has focused on individuals with a cancer diagnosis during childhood. Little is known about the specific impact of a cancer diagnosis with an onset in adolescence or the impact of childhood cancer on AYA psychosocial outcomes.
Evidence (psychosocial outcomes in AYA cancer survivors):
- Adult survivors of cancer diagnosed during adolescence (aged 15–18 years) (N = 825) were compared with an age-matched sample from the general population and a comparison group of adults without cancer.[142]
- Female survivors of adolescent cancers achieved fewer developmental milestones related to their psychosexual development, such as having their first boyfriend, or they reached these milestones later.
- Male survivors were more likely to live with their parents than were same-sex controls.
- Adolescent cancer survivors were less likely to have ever married or have had children. Survivors were significantly older at their first marriage and at the birth of their first child than were their age-matched samples.
- Survivors in this cohort were also significantly less satisfied with their general and health-related life than were people in a community-based control group. Impaired general and health-related life satisfaction were associated with somatic late effects, symptoms of depression and anxiety, and lower rates of posttraumatic growth.[143]
- A survey of 4,054 AYA cancer survivors and 345,592 respondents who had no history of cancer reported the following:[144]
- AYA cancer survivors were more likely to smoke (26% vs. 18%), be affected by obesity (31% vs. 27%), and have chronic conditions such as cardiovascular disease (14% vs. 7%), hypertension (35% vs. 9%), asthma (15% vs. 8%), disability (36% vs. 18%), and poor mental health (20% vs. 10%).
- They were also less likely to receive medical care because of cost (24% vs. 15%).
- The CCSS evaluated outcomes of 2,979 adolescent survivors and 649 siblings of childhood cancer survivors to determine the incidence of difficulty in six behavioral and social domains (depression/anxiety, being headstrong, attention deficit, peer conflict/social withdrawal, antisocial behaviors, and social competence).[145]
- Survivors were 1.5 times (95% CI, 1.1–2.1) more likely than siblings to have symptoms of depression/anxiety and 1.7 times (95% CI, 1.3–2.2) more likely than siblings to have antisocial behaviors.
- Scores in the depression/anxiety, attention deficit, and antisocial domains were significantly elevated in adolescents treated for leukemia or CNS tumors, compared with the scores in siblings.
- In addition, survivors of neuroblastoma had difficulty in the depression/anxiety and antisocial domains.
- CNS-directed treatments (cranial radiation therapy and/or intrathecal methotrexate) were specific risk factors for adverse behavioral outcomes.
- Another CCSS study evaluated psychological and neurocognitive function in 2,589 long-term cancer survivors who were diagnosed during adolescence and young adulthood.[146]
- Compared with a sibling cohort, survivors diagnosed during adolescence and young adulthood reported higher rates of depression (OR, 1.55; 95% CI, 1.04–2.30) and anxiety (OR, 2.00; 95% CI, 1.17–3.43) and reported more cognitive problems affecting task efficiency (OR, 1.72; 95% CI, 1.21–2.43), emotional regulation (OR, 1.74; 95% CI, 1.26–2.40), and memory (OR, 1.44; 95% CI, 1.09–1.89).
- Survivors of lymphoma and sarcoma diagnosed during later adolescence were at reduced risk of psychosocial and neurocognitive problems than were those diagnosed before age 11 years. These outcomes did not differ by age at diagnosis among CNS tumor and leukemia survivors.
- Survivors diagnosed during adolescence and young adulthood were also significantly less likely than sibling controls to have attained a post–high school education, be working full time, be married, or be living independently; inferior social outcomes were related to neurocognitive symptoms.
- A follow-up CCSS study evaluated profiles of symptom comorbidities in 3,993 adolescents (aged 13–17 years) treated for cancer.[147] Latent profile analysis identified four symptom profiles:
- No significant symptoms.
- Elevated internalizing symptoms (anxiety and/or depression, social withdrawal, and attention problems).
- Elevated externalizing symptoms (headstrong behavior and attention problems).
- Elevated internalizing and externalizing symptoms.
Overall results support that behavioral, emotional, and social symptoms frequently co-occur and are associated with treatment exposures (cranial radiation, corticosteroids, and methotrexate) and late effects (obesity, cancer-related pain, and sensory impairments) in adolescent survivors diagnosed between 1970 and 1986.
- Another CCSS study characterized the prevalence and risk of pain, clinically significant interference in daily activities because of pain, and recurrent pain in 10,012 adult survivors of childhood cancer (median time since diagnosis, 23 years).[148]
- A significant minority of survivors endorsed moderate to severe pain (29%), moderate to extreme pain interference (20%), and moderate to severe recurrent pain (9%).
- Older age at diagnosis and follow-up, female sex, and presence of grades 3 to 4 chronic medical conditions were consistently associated with an increased risk of worse pain outcomes.
- Minority racial and ethnic groups, diagnosis of CNS tumor, and treatment with platinum-based chemotherapy and cranial radiation were associated with an increased risk of late-occurrence pain and pain interference.
- Depression and anxiety were associated with increased risk of all pain outcomes, and poor vitality mediated the effects of anxiety on high pain and pain interference.
- An SJLIFE study evaluated the associations between comprehensive medical, neurocognitive, and physical performance assessments and self-reported pain, quality of life, and social functioning in 2,836 survivors (mean age, 32.2 years; mean time since diagnosis, 23.7 years) and 343 noncancer community controls.[149]
- Moderate-to-very-severe pain with moderate-to-extreme daily interference was endorsed by 18% of survivors, compared with 8% of controls (P < .001).
- Survivors of soft tissue sarcoma (OR, 9.25), non-Hodgkin lymphoma (OR, 4.13), and Ewing sarcoma and/or osteosarcoma (OR, 3.93) had the highest odds of pain with daily interference, compared with controls.
- In multivariable models that included treatment exposures, histories of amputation (OR, 1.89) and/or limb-sparing surgery (OR, 2.30) were associated with increased odds of pain with daily interference.
- Pain with daily interference was associated with an increased risk of impaired neurocognition (attention: RR, 1.88; memory: RR, 1.65) and physical functioning (aerobic capacity: RR, 2.29; mobility: RR, 1.71).
- Pain with daily interference was also associated with an increased risk of impaired social functioning (inability to hold a job and/or attend school: RR, 4.46; assistance with routine and/or personal care needs: RR, 5.64), and health-related quality of life (physical: RR, 6.34; emotional: RR, 2.83).
- A Nordic, register-based cohort study evaluated whether childhood cancer survivors (n = 18,621) were at a higher risk of developing psychiatric disorders later in life than their siblings (n = 24,775) and the general population (n = 88,630).[150]
- The cumulative incidence of contact with a psychiatric hospital by age 30 years was 15.9% for childhood cancer survivors, 14.0% for siblings, and 12.7% for matched (by birth year, sex, and country/municipality) population controls.
- The absolute difference was small, but survivors were still at a higher RR for any psychiatric hospital contact than their siblings (1.39) and matched controls (HR, 1.34).
- A CCSS study evaluated associations between treatment changes and neurocognition as well as the impact of neurocognition and chronic health conditions on adult independence in 1,284 adult survivors of childhood gliomas (median age, 30 years at assessment and 22 years from diagnosis).[151]
- Cranial radiation exposure decreased over the study period (1970s–1990s).
- Survivors with any treatment exposures (surgery only, chemotherapy with or without surgery, cranial radiation therapy with or without chemotherapy/surgery) had an elevated risk of neurocognitive impairment, compared with siblings.
- While most long-term glioma survivors in the cohort achieved adult independence, associations with treatment-related neurocognitive impairment and chronic health conditions were observed among those with functional nonindependence.
Evidence (functional and social independence):
- In a study of 665 survivors of CNS tumors (54% male; 52% treated with cranial radiation therapy; median age, 15 years; and 12 years from diagnosis), CCSS investigators observed the following:[117]
- Almost 50% of survivors experienced social difficulties related to peer relationships that exceeded those of survivors of solid tumors and sibling controls.
- Cranial radiation exposure predicted impaired social and peer relationships, and cognitive impairment mediated these associations.
- An SJLIFE study investigated functional and social independence in 306 CNS tumor survivors (astrocytoma [n = 130], medulloblastoma [n = 77], ependymoma [n = 36], and other [n = 63]; median age, 25 years; and time since diagnosis, 16.8 years).[49]
- Only 40% of long-term survivors in the study cohort achieved complete independence as adults.
- Predictors of nonindependence included treatment with craniospinal irradiation, history of hydrocephalus with shunting, and younger age at diagnosis.
- Beyond impaired IQ scores, functional limitations in aerobic capacity, flexibility, and adaptive physical function were significantly associated with nonindependence.
References:
- Grill J, Kieffer V, Kalifa C: Measuring the neuro-cognitive side-effects of irradiation in children with brain tumors. Pediatr Blood Cancer 42 (5): 452-6, 2004.
- Marusak HA, Iadipaolo AS, Harper FW, et al.: Neurodevelopmental consequences of pediatric cancer and its treatment: applying an early adversity framework to understanding cognitive, behavioral, and emotional outcomes. Neuropsychol Rev 28 (2): 123-175, 2018.
- Brinkman TM, Krasin MJ, Liu W, et al.: Long-Term Neurocognitive Functioning and Social Attainment in Adult Survivors of Pediatric CNS Tumors: Results From the St Jude Lifetime Cohort Study. J Clin Oncol 34 (12): 1358-67, 2016.
- Moxon-Emre I, Bouffet E, Taylor MD, et al.: Impact of craniospinal dose, boost volume, and neurologic complications on intellectual outcome in patients with medulloblastoma. J Clin Oncol 32 (17): 1760-8, 2014.
- Krull KR, Zhang N, Santucci A, et al.: Long-term decline in intelligence among adult survivors of childhood acute lymphoblastic leukemia treated with cranial radiation. Blood 122 (4): 550-3, 2013.
- Annett RD, Hile S, Bedrick E, et al.: Neuropsychological functioning of children treated for acute lymphoblastic leukemia: impact of whole brain radiation therapy. Psychooncology 24 (2): 181-9, 2015.
- van der Plas E, Qiu W, Nieman BJ, et al.: Sex-Specific Associations Between Chemotherapy, Chronic Conditions, and Neurocognitive Impairment in Acute Lymphoblastic Leukemia Survivors: A Report From the Childhood Cancer Survivor Study. J Natl Cancer Inst 113 (5): 588-596, 2021.
- Krull KR, Khan RB, Ness KK, et al.: Symptoms of attention-deficit/hyperactivity disorder in long-term survivors of childhood leukemia. Pediatr Blood Cancer 57 (7): 1191-6, 2011.
- Kahalley LS, Conklin HM, Tyc VL, et al.: ADHD and secondary ADHD criteria fail to identify many at-risk survivors of pediatric ALL and brain tumor. Pediatr Blood Cancer 57 (1): 110-8, 2011.
- Mahajan A, Stavinoha PL, Rongthong W, et al.: Neurocognitive Effects and Necrosis in Childhood Cancer Survivors Treated With Radiation Therapy: A PENTEC Comprehensive Review. Int J Radiat Oncol Biol Phys 119 (2): 401-416, 2024.
- Cheung YT, Brinkman TM, Li C, et al.: Chronic Health Conditions and Neurocognitive Function in Aging Survivors of Childhood Cancer: A Report from the Childhood Cancer Survivor Study. J Natl Cancer Inst 110 (4): 411-419, 2018.
- Bass JK, Liu W, Banerjee P, et al.: Association of Hearing Impairment With Neurocognition in Survivors of Childhood Cancer. JAMA Oncol 6 (9): 1363-1371, 2020.
- Barlow-Krelina E, Chen Y, Yasui Y, et al.: Consistent Physical Activity and Future Neurocognitive Problems in Adult Survivors of Childhood Cancers: A Report From the Childhood Cancer Survivor Study. J Clin Oncol 38 (18): 2041-2052, 2020.
- Bernal JDK, Recchia F, Yu DJ, et al.: Physical activity and exercise for cancer-related cognitive impairment among individuals affected by childhood cancer: a systematic review and meta-analysis. Lancet Child Adolesc Health 7 (1): 47-58, 2023.
- Phillips NS, Stratton KL, Williams AM, et al.: Late-onset Cognitive Impairment and Modifiable Risk Factors in Adult Childhood Cancer Survivors. JAMA Netw Open 6 (5): e2316077, 2023.
- Traunwieser T, Loos E, Ottensmeier H, et al.: Survivors of infant atypical teratoid/rhabdoid tumors present with severely impaired cognitive functions especially for fluid intelligence and visual processing: data from the German brain tumor studies. Pediatr Blood Cancer 71 (5): e30910, 2024.
- Merchant TE, Schreiber JE, Wu S, et al.: Critical combinations of radiation dose and volume predict intelligence quotient and academic achievement scores after craniospinal irradiation in children with medulloblastoma. Int J Radiat Oncol Biol Phys 90 (3): 554-61, 2014.
- Armstrong GT, Conklin HM, Huang S, et al.: Survival and long-term health and cognitive outcomes after low-grade glioma. Neuro Oncol 13 (2): 223-34, 2011.
- Di Pinto M, Conklin HM, Li C, et al.: Learning and memory following conformal radiation therapy for pediatric craniopharyngioma and low-grade glioma. Int J Radiat Oncol Biol Phys 84 (3): e363-9, 2012.
- Ris MD, Walsh K, Wallace D, et al.: Intellectual and academic outcome following two chemotherapy regimens and radiotherapy for average-risk medulloblastoma: COG A9961. Pediatr Blood Cancer 60 (8): 1350-7, 2013.
- Bowers DC, Liu Y, Leisenring W, et al.: Late-occurring stroke among long-term survivors of childhood leukemia and brain tumors: a report from the Childhood Cancer Survivor Study. J Clin Oncol 24 (33): 5277-82, 2006.
- Nassar SL, Conklin HM, Zhou Y, et al.: Neurocognitive outcomes among children who experienced seizures during treatment for acute lymphoblastic leukemia. Pediatr Blood Cancer 64 (8): , 2017.
- Torres VA, Ashford JM, Wright E, et al.: The impact of socioeconomic status (SES) on cognitive outcomes following radiotherapy for pediatric brain tumors: a prospective, longitudinal trial. Neuro Oncol 23 (7): 1173-1182, 2021.
- Mabbott DJ, Spiegler BJ, Greenberg ML, et al.: Serial evaluation of academic and behavioral outcome after treatment with cranial radiation in childhood. J Clin Oncol 23 (10): 2256-63, 2005.
- Brière ME, Scott JG, McNall-Knapp RY, et al.: Cognitive outcome in pediatric brain tumor survivors: delayed attention deficit at long-term follow-up. Pediatr Blood Cancer 50 (2): 337-40, 2008.
- Edelstein K, Spiegler BJ, Fung S, et al.: Early aging in adult survivors of childhood medulloblastoma: long-term neurocognitive, functional, and physical outcomes. Neuro Oncol 13 (5): 536-45, 2011.
- Palmer SL, Goloubeva O, Reddick WE, et al.: Patterns of intellectual development among survivors of pediatric medulloblastoma: a longitudinal analysis. J Clin Oncol 19 (8): 2302-8, 2001.
- Mulhern RK, Merchant TE, Gajjar A, et al.: Late neurocognitive sequelae in survivors of brain tumours in childhood. Lancet Oncol 5 (7): 399-408, 2004.
- Brinkman TM, Reddick WE, Luxton J, et al.: Cerebral white matter integrity and executive function in adult survivors of childhood medulloblastoma. Neuro Oncol 14 (Suppl 4): iv25-36, 2012.
- Jacola LM, Ashford JM, Reddick WE, et al.: The relationship between working memory and cerebral white matter volume in survivors of childhood brain tumors treated with conformal radiation therapy. J Neurooncol 119 (1): 197-205, 2014.
- Palmer SL, Glass JO, Li Y, et al.: White matter integrity is associated with cognitive processing in patients treated for a posterior fossa brain tumor. Neuro Oncol 14 (9): 1185-93, 2012.
- Ali JS, Ashford JM, Swain MA, et al.: Predictors of Cognitive Performance Among Infants Treated for Brain Tumors: Findings From a Multisite, Prospective, Longitudinal Trial. J Clin Oncol 39 (21): 2350-2358, 2021.
- Merchant TE, Conklin HM, Wu S, et al.: Late effects of conformal radiation therapy for pediatric patients with low-grade glioma: prospective evaluation of cognitive, endocrine, and hearing deficits. J Clin Oncol 27 (22): 3691-7, 2009.
- Liu APY, Hastings C, Wu S, et al.: Treatment burden and long-term health deficits of patients with low-grade gliomas or glioneuronal tumors diagnosed during the first year of life. Cancer 125 (7): 1163-1175, 2019.
- Palmer SL, Armstrong C, Onar-Thomas A, et al.: Processing speed, attention, and working memory after treatment for medulloblastoma: an international, prospective, and longitudinal study. J Clin Oncol 31 (28): 3494-500, 2013.
- Knight SJ, Conklin HM, Palmer SL, et al.: Working memory abilities among children treated for medulloblastoma: parent report and child performance. J Pediatr Psychol 39 (5): 501-11, 2014.
- Schreiber JE, Gurney JG, Palmer SL, et al.: Examination of risk factors for intellectual and academic outcomes following treatment for pediatric medulloblastoma. Neuro Oncol 16 (8): 1129-36, 2014.
- Khan RB, Patay Z, Klimo P, et al.: Clinical features, neurologic recovery, and risk factors of postoperative posterior fossa syndrome and delayed recovery: a prospective study. Neuro Oncol 23 (9): 1586-1596, 2021.
- Schreiber JE, Palmer SL, Conklin HM, et al.: Posterior fossa syndrome and long-term neuropsychological outcomes among children treated for medulloblastoma on a multi-institutional, prospective study. Neuro Oncol 19 (12): 1673-1682, 2017.
- Moxon-Emre I, Taylor MD, Bouffet E, et al.: Intellectual Outcome in Molecular Subgroups of Medulloblastoma. J Clin Oncol 34 (34): 4161-4170, 2016.
- Acharya S, Wu S, Ashford JM, et al.: Association between hippocampal dose and memory in survivors of childhood or adolescent low-grade glioma: a 10-year neurocognitive longitudinal study. Neuro Oncol 21 (9): 1175-1183, 2019.
- Ellenberg L, Liu Q, Gioia G, et al.: Neurocognitive status in long-term survivors of childhood CNS malignancies: a report from the Childhood Cancer Survivor Study. Neuropsychology 23 (6): 705-17, 2009.
- Armstrong GT, Liu Q, Yasui Y, et al.: Long-term outcomes among adult survivors of childhood central nervous system malignancies in the Childhood Cancer Survivor Study. J Natl Cancer Inst 101 (13): 946-58, 2009.
- Ris MD, Leisenring WM, Goodman P, et al.: Neuropsychological and socioeconomic outcomes in adult survivors of pediatric low-grade glioma. Cancer 125 (17): 3050-3058, 2019.
- Shabason EK, Brodsky C, Baran J, et al.: Clinical diagnosis of attention-deficit/hyperactivity disorder in survivors of pediatric brain tumors. J Neurooncol 143 (2): 305-312, 2019.
- Brinkman TM, Palmer SL, Chen S, et al.: Parent-reported social outcomes after treatment for pediatric embryonal tumors: a prospective longitudinal study. J Clin Oncol 30 (33): 4134-40, 2012.
- Moyer KH, Willard VW, Gross AM, et al.: The impact of attention on social functioning in survivors of pediatric acute lymphoblastic leukemia and brain tumors. Pediatr Blood Cancer 59 (7): 1290-5, 2012.
- Mitby PA, Robison LL, Whitton JA, et al.: Utilization of special education services and educational attainment among long-term survivors of childhood cancer: a report from the Childhood Cancer Survivor Study. Cancer 97 (4): 1115-26, 2003.
- Brinkman TM, Ness KK, Li Z, et al.: Attainment of Functional and Social Independence in Adult Survivors of Pediatric CNS Tumors: A Report From the St Jude Lifetime Cohort Study. J Clin Oncol 36 (27): 2762-2769, 2018.
- Kahalley LS, Ris MD, Grosshans DR, et al.: Comparing Intelligence Quotient Change After Treatment With Proton Versus Photon Radiation Therapy for Pediatric Brain Tumors. J Clin Oncol 34 (10): 1043-9, 2016.
- Pulsifer MB, Sethi RV, Kuhlthau KA, et al.: Early Cognitive Outcomes Following Proton Radiation in Pediatric Patients With Brain and Central Nervous System Tumors. Int J Radiat Oncol Biol Phys 93 (2): 400-7, 2015.
- Kahalley LS, Peterson R, Ris MD, et al.: Superior Intellectual Outcomes After Proton Radiotherapy Compared With Photon Radiotherapy for Pediatric Medulloblastoma. J Clin Oncol 38 (5): 454-461, 2020.
- Reddick WE, Glass JO, Helton KJ, et al.: Prevalence of leukoencephalopathy in children treated for acute lymphoblastic leukemia with high-dose methotrexate. AJNR Am J Neuroradiol 26 (5): 1263-9, 2005.
- Waber DP, Queally JT, Catania L, et al.: Neuropsychological outcomes of standard risk and high risk patients treated for acute lymphoblastic leukemia on Dana-Farber ALL consortium protocol 95-01 at 5 years post-diagnosis. Pediatr Blood Cancer 58 (5): 758-65, 2012.
- Krull KR, Brinkman TM, Li C, et al.: Neurocognitive outcomes decades after treatment for childhood acute lymphoblastic leukemia: a report from the St Jude lifetime cohort study. J Clin Oncol 31 (35): 4407-15, 2013.
- Reddick WE, Shan ZY, Glass JO, et al.: Smaller white-matter volumes are associated with larger deficits in attention and learning among long-term survivors of acute lymphoblastic leukemia. Cancer 106 (4): 941-9, 2006.
- Kadan-Lottick NS, Zeltzer LK, Liu Q, et al.: Neurocognitive functioning in adult survivors of childhood non-central nervous system cancers. J Natl Cancer Inst 102 (12): 881-93, 2010.
- Schuitema I, Deprez S, Van Hecke W, et al.: Accelerated aging, decreased white matter integrity, and associated neuropsychological dysfunction 25 years after pediatric lymphoid malignancies. J Clin Oncol 31 (27): 3378-88, 2013.
- Armstrong GT, Reddick WE, Petersen RC, et al.: Evaluation of memory impairment in aging adult survivors of childhood acute lymphoblastic leukemia treated with cranial radiotherapy. J Natl Cancer Inst 105 (12): 899-907, 2013.
- Spiegler BJ, Kennedy K, Maze R, et al.: Comparison of long-term neurocognitive outcomes in young children with acute lymphoblastic leukemia treated with cranial radiation or high-dose or very high-dose intravenous methotrexate. J Clin Oncol 24 (24): 3858-64, 2006.
- Campbell LK, Scaduto M, Sharp W, et al.: A meta-analysis of the neurocognitive sequelae of treatment for childhood acute lymphocytic leukemia. Pediatr Blood Cancer 49 (1): 65-73, 2007.
- Cheung YT, Sabin ND, Reddick WE, et al.: Leukoencephalopathy and long-term neurobehavioural, neurocognitive, and brain imaging outcomes in survivors of childhood acute lymphoblastic leukaemia treated with chemotherapy: a longitudinal analysis. Lancet Haematol 3 (10): e456-e466, 2016.
- Jansen NC, Kingma A, Schuitema A, et al.: Neuropsychological outcome in chemotherapy-only-treated children with acute lymphoblastic leukemia. J Clin Oncol 26 (18): 3025-30, 2008.
- Iyer NS, Balsamo LM, Bracken MB, et al.: Chemotherapy-only treatment effects on long-term neurocognitive functioning in childhood ALL survivors: a review and meta-analysis. Blood 126 (3): 346-53, 2015.
- Jacola LM, Krull KR, Pui CH, et al.: Longitudinal Assessment of Neurocognitive Outcomes in Survivors of Childhood Acute Lymphoblastic Leukemia Treated on a Contemporary Chemotherapy Protocol. J Clin Oncol 34 (11): 1239-47, 2016.
- Espy KA, Moore IM, Kaufmann PM, et al.: Chemotherapeutic CNS prophylaxis and neuropsychologic change in children with acute lymphoblastic leukemia: a prospective study. J Pediatr Psychol 26 (1): 1-9, 2001 Jan-Feb.
- Buizer AI, de Sonneville LM, Veerman AJ: Effects of chemotherapy on neurocognitive function in children with acute lymphoblastic leukemia: a critical review of the literature. Pediatr Blood Cancer 52 (4): 447-54, 2009.
- Gandy K, Sapkota Y, Scoggins MA, et al.: Genetic variants, neurocognitive outcomes, and functional neuroimaging in survivors of childhood acute lymphoblastic leukemia. JNCI Cancer Spectr 7 (4): , 2023.
- Cole PD, Finkelstein Y, Stevenson KE, et al.: Polymorphisms in Genes Related to Oxidative Stress Are Associated With Inferior Cognitive Function After Therapy for Childhood Acute Lymphoblastic Leukemia. J Clin Oncol 33 (19): 2205-11, 2015.
- Jacola LM, Edelstein K, Liu W, et al.: Cognitive, behaviour, and academic functioning in adolescent and young adult survivors of childhood acute lymphoblastic leukaemia: a report from the Childhood Cancer Survivor Study. Lancet Psychiatry 3 (10): 965-972, 2016.
- Jacola LM, Conklin HM, Krull KR, et al.: The Impact of Intensified CNS-Directed Therapy on Neurocognitive Outcomes in Survivors of Childhood Acute Lymphoblastic Leukemia Treated Without Cranial Irradiation. J Clin Oncol 40 (36): 4218-4227, 2022.
- Krull KR, Cheung YT, Liu W, et al.: Chemotherapy Pharmacodynamics and Neuroimaging and Neurocognitive Outcomes in Long-Term Survivors of Childhood Acute Lymphoblastic Leukemia. J Clin Oncol 34 (22): 2644-53, 2016.
- Halsey C, Buck G, Richards S, et al.: The impact of therapy for childhood acute lymphoblastic leukaemia on intelligence quotients; results of the risk-stratified randomized central nervous system treatment trial MRC UKALL XI. J Hematol Oncol 4: 42, 2011.
- Kadan-Lottick NS, Brouwers P, Breiger D, et al.: A comparison of neurocognitive functioning in children previously randomized to dexamethasone or prednisone in the treatment of childhood acute lymphoblastic leukemia. Blood 114 (9): 1746-52, 2009.
- Williams AM, Cheung YT, Hyun G, et al.: Childhood Neurotoxicity and Brain Resilience to Adverse Events during Adulthood. Ann Neurol 89 (3): 534-545, 2021.
- Stefanski KJ, Anixt JS, Goodman P, et al.: Long-Term Neurocognitive and Psychosocial Outcomes After Acute Myeloid Leukemia: A Childhood Cancer Survivor Study Report. J Natl Cancer Inst 113 (4): 481-495, 2021.
- Edelmann MN, Daryani VM, Bishop MW, et al.: Neurocognitive and Patient-Reported Outcomes in Adult Survivors of Childhood Osteosarcoma. JAMA Oncol 2 (2): 201-8, 2016.
- van der Plas E, Darji H, Srivastava DK, et al.: Risk factors for neurocognitive impairment, emotional distress, and poor quality of life in survivors of pediatric rhabdomyosarcoma: A report from the Childhood Cancer Survivor Study. Cancer 130 (12): 2224-2236, 2024.
- Tonning Olsson I, Brinkman TM, Wang M, et al.: Neurocognitive and psychosocial outcomes in adult survivors of childhood soft-tissue sarcoma: A report from the St. Jude Lifetime Cohort. Cancer 126 (7): 1576-1584, 2020.
- Tonning Olsson I, Brinkman TM, Hyun G, et al.: Neurocognitive outcomes in long-term survivors of Wilms tumor: a report from the St. Jude Lifetime Cohort. J Cancer Surviv 13 (4): 570-579, 2019.
- Willard VW, Qaddoumi I, Chen S, et al.: Developmental and adaptive functioning in children with retinoblastoma: a longitudinal investigation. J Clin Oncol 32 (25): 2788-93, 2014.
- Willard VW, Qaddoumi I, Pan H, et al.: Cognitive and Adaptive Functioning in Youth With Retinoblastoma: A Longitudinal Investigation Through 10 Years of Age. J Clin Oncol 39 (24): 2676-2684, 2021.
- Brinkman TM, Merchant TE, Li Z, et al.: Cognitive function and social attainment in adult survivors of retinoblastoma: a report from the St. Jude Lifetime Cohort Study. Cancer 121 (1): 123-31, 2015.
- Ehrhardt MJ, Sandlund JT, Zhang N, et al.: Late outcomes of adult survivors of childhood non-Hodgkin lymphoma: A report from the St. Jude Lifetime Cohort Study. Pediatr Blood Cancer 64 (6): , 2017.
- Krull KR, Sabin ND, Reddick WE, et al.: Neurocognitive function and CNS integrity in adult survivors of childhood hodgkin lymphoma. J Clin Oncol 30 (29): 3618-24, 2012.
- Hesko C, Liu W, Srivastava DK, et al.: Neurocognitive outcomes in adult survivors of neuroblastoma: A report from the Childhood Cancer Survivor Study. Cancer 129 (18): 2904-2914, 2023.
- Wu NL, Phipps AI, Krull KR, et al.: Long-term patient-reported neurocognitive outcomes in adult survivors of hematopoietic cell transplant. Blood Adv 6 (14): 4347-4356, 2022.
- Willard VW, Leung W, Huang Q, et al.: Cognitive outcome after pediatric stem-cell transplantation: impact of age and total-body irradiation. J Clin Oncol 32 (35): 3982-8, 2014.
- Kenborg L, Winther JF, Linnet KM, et al.: Neurologic disorders in 4858 survivors of central nervous system tumors in childhood-an Adult Life after Childhood Cancer in Scandinavia (ALiCCS) study. Neuro Oncol 21 (1): 125-136, 2019.
- Wells EM, Ullrich NJ, Seidel K, et al.: Longitudinal assessment of late-onset neurologic conditions in survivors of childhood central nervous system tumors: a Childhood Cancer Survivor Study report. Neuro Oncol 20 (1): 132-142, 2018.
- Goldsby RE, Liu Q, Nathan PC, et al.: Late-occurring neurologic sequelae in adult survivors of childhood acute lymphoblastic leukemia: a report from the Childhood Cancer Survivor Study. J Clin Oncol 28 (2): 324-31, 2010.
- Phillips NS, Khan RB, Li C, et al.: Seizures' impact on cognition and quality of life in childhood cancer survivors. Cancer 128 (1): 180-191, 2022.
- Jain P, Gulati S, Seth R, et al.: Vincristine-induced neuropathy in childhood ALL (acute lymphoblastic leukemia) survivors: prevalence and electrophysiological characteristics. J Child Neurol 29 (7): 932-7, 2014.
- Ness KK, Jones KE, Smith WA, et al.: Chemotherapy-related neuropathic symptoms and functional impairment in adult survivors of extracranial solid tumors of childhood: results from the St. Jude Lifetime Cohort Study. Arch Phys Med Rehabil 94 (8): 1451-7, 2013.
- Kandula T, Farrar MA, Cohn RJ, et al.: Chemotherapy-Induced Peripheral Neuropathy in Long-term Survivors of Childhood Cancer: Clinical, Neurophysiological, Functional, and Patient-Reported Outcomes. JAMA Neurol 75 (8): 980-988, 2018.
- Rodwin RL, Ross WL, Rotatori J, et al.: Newly identified chemotherapy-induced peripheral neuropathy in a childhood cancer survivorship clinic. Pediatr Blood Cancer 69 (3): e29550, 2022.
- Varedi M, Lu L, Howell CR, et al.: Peripheral Neuropathy, Sensory Processing, and Balance in Survivors of Acute Lymphoblastic Leukemia. J Clin Oncol 36 (22): 2315-2322, 2018.
- Gurney JG, Kadan-Lottick NS, Packer RJ, et al.: Endocrine and cardiovascular late effects among adult survivors of childhood brain tumors: Childhood Cancer Survivor Study. Cancer 97 (3): 663-73, 2003.
- Ullrich NJ, Robertson R, Kinnamon DD, et al.: Moyamoya following cranial irradiation for primary brain tumors in children. Neurology 68 (12): 932-8, 2007.
- Wang C, Roberts KB, Bindra RS, et al.: Delayed cerebral vasculopathy following cranial radiation therapy for pediatric tumors. Pediatr Neurol 50 (6): 549-56, 2014.
- Mueller S, Fullerton HJ, Stratton K, et al.: Radiation, atherosclerotic risk factors, and stroke risk in survivors of pediatric cancer: a report from the Childhood Cancer Survivor Study. Int J Radiat Oncol Biol Phys 86 (4): 649-55, 2013.
- Reulen RC, Guha J, Bright CJ, et al.: Risk of cerebrovascular disease among 13 457 five-year survivors of childhood cancer: A population-based cohort study. Int J Cancer 148 (3): 572-583, 2021.
- Fullerton HJ, Stratton K, Mueller S, et al.: Recurrent stroke in childhood cancer survivors. Neurology 85 (12): 1056-64, 2015.
- Waxer JF, Wong K, Modiri A, et al.: Risk of Cerebrovascular Events Among Childhood and Adolescent Patients Receiving Cranial Radiation Therapy: A PENTEC Normal Tissue Outcomes Comprehensive Review. Int J Radiat Oncol Biol Phys 119 (2): 417-430, 2024.
- Khan RB, Merchant TE, Sadighi ZS, et al.: Prevalence, risk factors, and response to treatment for hypersomnia of central origin in survivors of childhood brain tumors. J Neurooncol 136 (2): 379-384, 2018.
- van Kooten JAMC, Maurice-Stam H, Schouten AYN, et al.: High occurrence of sleep problems in survivors of a childhood brain tumor with neurocognitive complaints: The association with psychosocial and behavioral executive functioning. Pediatr Blood Cancer 66 (11): e27947, 2019.
- Khan RB, Hudson MM, Ledet DS, et al.: Neurologic morbidity and quality of life in survivors of childhood acute lymphoblastic leukemia: a prospective cross-sectional study. J Cancer Surviv 8 (4): 688-96, 2014.
- Khong PL, Leung LH, Fung AS, et al.: White matter anisotropy in post-treatment childhood cancer survivors: preliminary evidence of association with neurocognitive function. J Clin Oncol 24 (6): 884-90, 2006.
- Zeller B, Tamnes CK, Kanellopoulos A, et al.: Reduced neuroanatomic volumes in long-term survivors of childhood acute lymphoblastic leukemia. J Clin Oncol 31 (17): 2078-85, 2013.
- Faraci M, Morana G, Bagnasco F, et al.: Magnetic resonance imaging in childhood leukemia survivors treated with cranial radiotherapy: a cross sectional, single center study. Pediatr Blood Cancer 57 (2): 240-6, 2011.
- Phillips NS, Hillenbrand CM, Mitrea BG, et al.: Cerebral microbleeds in adult survivors of childhood acute lymphoblastic leukemia treated with cranial radiation. Sci Rep 10 (1): 692, 2020.
- Rodwin RL, Chen Y, Yasui Y, et al.: Longitudinal Evaluation of Neuromuscular Dysfunction in Long-term Survivors of Childhood Cancer: A Report from the Childhood Cancer Survivor Study. Cancer Epidemiol Biomarkers Prev 30 (8): 1536-1545, 2021.
- Rodwin RL, Wang F, Lu L, et al.: Motor and sensory impairment in survivors of childhood central nervous system (CNS) tumors in the St. Jude Lifetime Cohort (SJLIFE). Cancer Med 13 (14): e7422, 2024.
- Cooper BT, Mayo CS, Milano MT, et al.: Predictive Factors Associated With Radiation Myelopathy in Pediatric Patients With Cancer: A PENTEC Comprehensive Review. Int J Radiat Oncol Biol Phys 119 (2): 494-506, 2024.
- Ness KK, Hudson MM, Jones KE, et al.: Effect of Temporal Changes in Therapeutic Exposure on Self-reported Health Status in Childhood Cancer Survivors. Ann Intern Med 166 (2): 89-98, 2017.
- Ernst M, Hinz A, Brähler E, et al.: Quality of life after pediatric cancer: comparison of long-term childhood cancer survivors' quality of life with a representative general population sample and associations with physical health and risk indicators. Health Qual Life Outcomes 21 (1): 65, 2023.
- Schulte F, Brinkman TM, Li C, et al.: Social adjustment in adolescent survivors of pediatric central nervous system tumors: A report from the Childhood Cancer Survivor Study. Cancer 124 (17): 3596-3608, 2018.
- Vuotto SC, Wang M, Okcu MF, et al.: Neurologic morbidity and functional independence in adult survivors of childhood cancer. Ann Clin Transl Neurol 11 (2): 291-301, 2024.
- Hörnquist L, Rickardsson J, Lannering B, et al.: Altered self-perception in adult survivors treated for a CNS tumor in childhood or adolescence: population-based outcomes compared with the general population. Neuro Oncol 17 (5): 733-40, 2015.
- Schulte F, Barrera M: Social competence in childhood brain tumor survivors: a comprehensive review. Support Care Cancer 18 (12): 1499-513, 2010.
- Papini C, Willard VW, Gajjar A, et al.: Social cognition and adjustment in adult survivors of pediatric central nervous system tumors. Cancer 129 (19): 3064-3075, 2023.
- Bonneau J, Berbis J, Michel G, et al.: Adolescence and Socioeconomic Factors: Key Factors in the Long-Term Impact of Leukemia on Scholastic Performance-A LEA Study. J Pediatr 205: 168-175.e2, 2019.
- Drabbe C, Coenraadts ES, van Houdt WJ, et al.: Impaired social functioning in adolescent and young adult sarcoma survivors: Prevalence and risk factors. Cancer 129 (9): 1419-1431, 2023.
- Ernst M, Brähler E, Wild PS, et al.: Risk factors for suicidal ideation in a large, registry-based sample of adult long-term childhood cancer survivors. J Affect Disord 265: 351-356, 2020.
- Lubas MM, Mirzaei Salehabadi S, Lavecchia J, et al.: Suicidality among adult survivors of childhood cancer: A report from the St. Jude Lifetime Cohort Study. Cancer 126 (24): 5347-5355, 2020.
- Brinkman TM, Zhang N, Recklitis CJ, et al.: Suicide ideation and associated mortality in adult survivors of childhood cancer. Cancer 120 (2): 271-7, 2014.
- Gunnes MW, Lie RT, Bjørge T, et al.: Suicide and violent deaths in survivors of cancer in childhood, adolescence and young adulthood-A national cohort study. Int J Cancer 140 (3): 575-580, 2017.
- Sun CL, Francisco L, Baker KS, et al.: Adverse psychological outcomes in long-term survivors of hematopoietic cell transplantation: a report from the Bone Marrow Transplant Survivor Study (BMTSS). Blood 118 (17): 4723-31, 2011.
- Vuotto SC, Krull KR, Li C, et al.: Impact of chronic disease on emotional distress in adult survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. Cancer 123 (3): 521-528, 2017.
- Zheng DJ, Krull KR, Chen Y, et al.: Long-term psychological and educational outcomes for survivors of neuroblastoma: A report from the Childhood Cancer Survivor Study. Cancer 124 (15): 3220-3230, 2018.
- Recklitis C, O'Leary T, Diller L: Utility of routine psychological screening in the childhood cancer survivor clinic. J Clin Oncol 21 (5): 787-92, 2003.
- Hsu TW, Liang CS, Tsai SJ, et al.: Risk of Major Psychiatric Disorders Among Children and Adolescents Surviving Malignancies: A Nationwide Longitudinal Study. J Clin Oncol 41 (11): 2054-2066, 2023.
- De R, Sutradhar R, Kurdyak P, et al.: Incidence and Predictors of Mental Health Outcomes Among Survivors of Adolescent and Young Adult Cancer: A Population-Based Study Using the IMPACT Cohort. J Clin Oncol 39 (9): 1010-1019, 2021.
- Phipps S, Klosky JL, Long A, et al.: Posttraumatic stress and psychological growth in children with cancer: has the traumatic impact of cancer been overestimated? J Clin Oncol 32 (7): 641-6, 2014.
- Stuber ML, Meeske KA, Leisenring W, et al.: Defining medical posttraumatic stress among young adult survivors in the Childhood Cancer Survivor Study. Gen Hosp Psychiatry 33 (4): 347-53, 2011 Jul-Aug.
- Phipps S, Larson S, Long A, et al.: Adaptive style and symptoms of posttraumatic stress in children with cancer and their parents. J Pediatr Psychol 31 (3): 298-309, 2006.
- Phipps S, Jurbergs N, Long A: Symptoms of post-traumatic stress in children with cancer: does personality trump health status? Psychooncology 18 (9): 992-1002, 2009.
- Rourke MT, Hobbie WL, Schwartz L, et al.: Posttraumatic stress disorder (PTSD) in young adult survivors of childhood cancer. Pediatr Blood Cancer 49 (2): 177-82, 2007.
- Schwartz L, Drotar D: Posttraumatic stress and related impairment in survivors of childhood cancer in early adulthood compared to healthy peers. J Pediatr Psychol 31 (4): 356-66, 2006.
- Stuber ML, Meeske KA, Krull KR, et al.: Prevalence and predictors of posttraumatic stress disorder in adult survivors of childhood cancer. Pediatrics 125 (5): e1124-34, 2010.
- Hobbie WL, Stuber M, Meeske K, et al.: Symptoms of posttraumatic stress in young adult survivors of childhood cancer. J Clin Oncol 18 (24): 4060-6, 2000.
- Dieluweit U, Debatin KM, Grabow D, et al.: Social outcomes of long-term survivors of adolescent cancer. Psychooncology 19 (12): 1277-84, 2010.
- Seitz DC, Hagmann D, Besier T, et al.: Life satisfaction in adult survivors of cancer during adolescence: what contributes to the latter satisfaction with life? Qual Life Res 20 (2): 225-36, 2011.
- Tai E, Buchanan N, Townsend J, et al.: Health status of adolescent and young adult cancer survivors. Cancer 118 (19): 4884-91, 2012.
- Schultz KA, Ness KK, Whitton J, et al.: Behavioral and social outcomes in adolescent survivors of childhood cancer: a report from the childhood cancer survivor study. J Clin Oncol 25 (24): 3649-56, 2007.
- Prasad PK, Hardy KK, Zhang N, et al.: Psychosocial and Neurocognitive Outcomes in Adult Survivors of Adolescent and Early Young Adult Cancer: A Report From the Childhood Cancer Survivor Study. J Clin Oncol 33 (23): 2545-52, 2015.
- Brinkman TM, Li C, Vannatta K, et al.: Behavioral, Social, and Emotional Symptom Comorbidities and Profiles in Adolescent Survivors of Childhood Cancer: A Report From the Childhood Cancer Survivor Study. J Clin Oncol 34 (28): 3417-25, 2016.
- Karlson CW, Alberts NM, Liu W, et al.: Longitudinal pain and pain interference in long-term survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. Cancer 126 (12): 2915-2923, 2020.
- Tonning Olsson I, Alberts NM, Li C, et al.: Pain and functional outcomes in adult survivors of childhood cancer: A report from the St. Jude Lifetime Cohort study. Cancer 127 (10): 1679-1689, 2021.
- Frederiksen LE, Erdmann F, Mader L, et al.: Psychiatric disorders in childhood cancer survivors in Denmark, Finland, and Sweden: a register-based cohort study from the SALiCCS research programme. Lancet Psychiatry 9 (1): 35-45, 2022.
- Papini C, Mirzaei S S, Xing M, et al.: Evolving therapies, neurocognitive outcomes, and functional independence in adult survivors of childhood glioma. J Natl Cancer Inst 116 (2): 288-298, 2024.
Late Effects of the Endocrine System
Endocrine dysfunction is common among survivors of childhood cancer, especially in those who were treated with surgery or radiation therapy that involved hormone-producing organs and those who received alkylating agent chemotherapy.
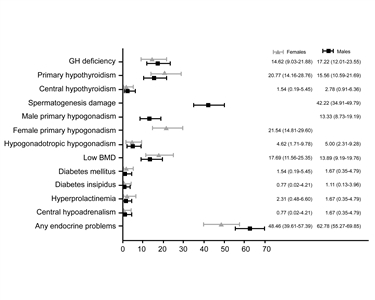
Figure 6. Prevalence of endocrine disorders at the last follow-up visit, by sex. Brignardello E, Felicetti F, Castiglione A, et al.: Endocrine health conditions in adult survivors of childhood cancer: the need for specialized adult-focused follow-up clinics. European Journal of Endocrinology 168 (3): 465-472, 2013. Copyright © 2013, European Society of Endocrinology.
The prevalence of specific endocrine disorders is affected by the following:[1,2,3,4]
- Patient factors (e.g., age at treatment and sex).
- Tumor location (e.g., suprasellar and nonsuprasellar).[5]
- Treatment factors (e.g., radiation dose and treatment volume).
- Time from radiation exposure (typically increases with longer time from radiation exposure [see Figure 6]).[1]
Endocrinologic late effects can be broadly categorized as those resulting from hypothalamic-pituitary injury or from peripheral glandular compromise.[1,2,3,4] The former are most common after treatment for central nervous system (CNS) tumors. The prevalence of these late effects was 24.8% in a nationwide cohort study of 718 survivors who lived longer than 2 years and all hypothalamic-pituitary axes were affected.[3]
The following sections summarize research that characterizes the clinical features of survivors at risk of endocrine dysfunction that impacts pituitary, thyroid, adrenal, and gonadal function.
Thyroid Gland
- Thyroid dysfunction is a common delayed effect after radiation therapy exposures to fields that include the thyroid gland. This type of radiation therapy is used in treating Hodgkin lymphoma, brain tumors, head and neck sarcomas, and acute lymphoblastic leukemia (ALL).
- There is considerable evidence linking radiation exposure to thyroid abnormalities. However, the prevalence of specific conditions varies widely because studies are limited by cohort selection and participation bias, heterogeneity in radiation treatment approach, time since radiation exposure, and method of ascertainment (e.g., self-report vs. clinical or diagnostic imaging assessment).
- Thyroid abnormalities observed in excess in childhood cancer survivors include the following:
- Primary hypothyroidism.
- Hyperthyroidism.
- Goiter.
- Nodules.
Hypothyroidism
Risk factors
Thyroid radiation therapy. An increased risk of hypothyroidism has been reported among childhood cancer survivors treated with head and neck radiation exposing the thyroid gland, especially among survivors of Hodgkin lymphoma.[1,2,3,4] Among survivors of head and neck tumors treated with radiation therapy potentially exposing the hypothalamic-pituitary region and the thyroid gland, hypothyroidism may result from thyrotropin-releasing hormone (TRH) and/or thyroid-stimulating hormone (TSH) deficiency (central hypothyroidism), thyroid gland dysfunction (primary hypothyroidism), or a combination of central and primary causes.
Iodine I 131-metaiodobenzylguanidine (131I-MIBG).
- Therapeutic 131I-MIBG. Thyroid disorders, including primary hypothyroidism, have been reported in children with neuroblastoma who were treated with 131I-MIBG, despite thyroid protection with potassium iodide, perchlorate, or the combination of potassium iodide, thyroxine (T4), and a thiamazole. However, these reports feature small numbers of patients who have other treatment-related risk factors for thyroid disorders, which limits the ability to identify an independent effect of 131I-MIBG.[6] Thyroid disorders were diagnosed in 81% of survivors 15 years after treatment with 131I-MIBG.[7]
- Diagnostic 131I-MIBG. Late-onset thyroid abnormalities have not been reported among childhood cancer survivors who had either 131I-MIBG or 123I-MIBG to monitor disease status.[8,9]
- A retrospective cohort study (n = 48) assessed the prevalence of thyroid dysfunction in survivors of a neuroblastic tumor who received 123I-MIBG for diagnostic purposes. All patients received thyroid prophylaxis (potassium iodide or combination of potassium iodide, thiamazole, and T4) during exposure to 123I-MIBG. After a median follow up of 6.6 years, thyroid function was normal in 46 of the 48 survivors. Two survivors had mild thyroid dysfunction.[10]
Thyroidectomy. As observed in the general, noncancer population, partial or obviously subtotal surgical resection of the thyroid is a risk factor for subsequent hypothyroidism.[11,12,13]
Evidence (prevalence of and risk factors for hypothyroidism):
- The German Group of Paediatric Radiation Oncology reported on 1,086 patients treated at 62 centers, including 404 patients (median age, 10.9 years) who received radiation therapy to the thyroid and/or pituitary gland.[14] Follow-up information was available for 264 patients (60.9%; median follow-up, 40 months), with 60 patients (22.7%) showing pathological values.
- Compared with patients treated with prophylactic cranial irradiation (median dose, 12 Gy), the hazard ratio (HR) for the development of pathological thyroid blood values was 3.072 (P = .002) for patients treated with radiation doses of 15 Gy to 25 Gy to the thyroid gland.
- The HR was 3.769 (P = .009) for patients treated with more than 25 Gy of radiation to the thyroid gland. The HR was 5.674 (P < .001) for patients treated with craniospinal irradiation (CSI).
- The cumulative incidence of thyroid hormone substitution therapy did not differ between defined subgroups.
- The Childhood Cancer Survivor Study (CCSS) investigated the prevalence of self-reported hypothyroidism assessed through serial questionnaires in 12,015 survivors. A total of 1,193 cases of hypothyroidism were observed, 777 (65%) of which occurred 5 or more years after a cancer diagnosis.[15]
- The prevalence at 5 years after a cancer diagnosis and the incidence through 30 years after a cancer diagnosis was the highest in 5-year survivors of Hodgkin lymphoma (32.3%) and CNS tumors (17.7%).
- The incidence was significantly associated with radiation dose to the thyroid and pituitary. The combined effects of thyroid and hypothalamic-pituitary doses appear to be less than additive when pituitary doses are greater than 16 Gy.
- Radiation-related risks were higher in males than females and inversely associated with age at exposure and time since exposure but remained elevated more than 25 years after exposure.
- Certain types of chemotherapy were significantly associated with the risk: bleomycin (rate ratio, 3.4), and the alkylating agents lomustine (rate ratio, 3.0) and cyclophosphamide (rate ratio, 1.3). The strongest chemotherapy-associated risk occurred among survivors of CNS cancer. A significant dose response for lomustine was observed (P < .01).
- In the CCSS, a cohort of childhood Hodgkin lymphoma survivors treated between 1970 and 1986 were evaluated for thyroid disease by use of a self-report questionnaire.[16]
- Among 1,791 survivors who were followed for a median of 14 years, 34% reported that they had been diagnosed with at least one thyroid abnormality.
- For hypothyroidism, there was a clear dose response, with a 20-year risk of:
- 20% for those who received less than 35 Gy of radiation to the thyroid gland.
- 30% for those who received 35 Gy to 44.9 Gy of radiation to the thyroid gland.
- 50% for those who received more than 45 Gy of radiation to the thyroid gland.
- Compared with a sibling control group, the relative risk (RR) was 17.1 for hypothyroidism.
- Elapsed time since diagnosis was a risk factor for hypothyroidism, with the risk increasing in the first 3 to 5 years postdiagnosis.
- Females were at increased risk for hypothyroidism.
- A follow-up study from the CCSS compared self-reported data from 14,290 survivors with data from 4,031 sibling controls.[2]
- The RR was 3.8 for hypothyroidism and remained significantly higher in survivors when compared with controls, even in the absence of radiation therapy to the thyroid or pituitary.
- These results indicate the need for continued and individualized long-term monitoring strategies in childhood cancer survivors.
- Continuous improvements in the precision of radiation therapy delivery carry the promise to decrease the radiation therapy dose received by the thyroid in a subset of patients. This was demonstrated in a study of 189 children and young adults (aged <26 years) with brain tumors treated with proton radiation therapy.[17]
- At a median follow-up of 4.4 years, the cumulative incidence of primary hypothyroidism was 3% after CSI and 1.6% overall, which is substantially lower than previous reports of 56% to 65% incidence after CSI with photons.
- Among 118 survivors of medulloblastoma (median follow-up, 5.6 years), the estimated cumulative incidence of hypothyroidism was 35.8% (95% confidence interval [CI], 26.7%–47.1%) by 5 years after radiation therapy.[18]
- The median time from the end of radiation therapy to the development of hypothyroidism was 2.1 years (range, 0.1–7.1 years) after proton radiation therapy and 2.9 years (range, 0.8–7.2 years) after photon radiation therapy.
- The rate of hypothyroidism (HR, 2.36; 95% CI, 1.11–5.02) was higher among patients treated with photon radiation therapy compared with those treated with proton radiation therapy.
- Differences in hypothyroidism risk by radiation modality were largely attributed to higher rates of primary hypothyroidism after photon radiation therapy (HR, 4.61; 95% CI, 1.20–17.66).
- St. Jude Life (SJLIFE) cohort study investigators evaluated the prevalence of and risk factors for primary hypothyroidism and its associations with chronic health conditions and quality of life among 2,965 childhood cancer survivors (median age, 30.9 years; median time postdiagnosis, 22.3 years).[13]
- Primary hypothyroidism was prevalent in 14.7% of survivors. It was more common in females (odds ratio [OR], 1.06; 95% CI, 1.03–1.08) and survivors diagnosed older than 15 years (vs. age <5 years). It was less common in non-White survivors (OR, 0.96; 95% CI, 0.93–0.99).
- Radiation therapy potentially exposing the thyroid gland was associated with dose-related risk of hypothyroidism.
- Significant associations with primary hypothyroidism included frailty (OR, 1.54; 95% CI, 1.05–2.26), dyslipidemia (OR, 1.52; 95% CI, 1.14–2.04), and impaired physical quality of life (OR, 1.66; 95% CI, 1.12–2.48).
- The Pediatric Normal Tissue Effects in the Clinic (PENTEC) research consortium performed a systematic review of radiation-associated primary hypothyroidism in children younger than 21 years between 1970 and 2017.[19]
- At mean doses of 10 Gy, 20 Gy, and 30 Gy, predicted rates of uncompensated (clinical) hypothyroidism were 4%, 7%, and 13%, respectively. The compensated (subclinical) hypothyroidism rates were 12%, 25% and 44%, respectively.
- Female sex (RR, 1.7; P < .0001) and age younger than 15 years at the time of radiation therapy (RR, 1.3; P < .005) were associated with higher risks of hypothyroidism.
- After a mean thyroid dose of 20 Gy, predicted rates of hypothyroidism were 13% for males younger than 14 years and more than 29% for females older than 15 years at the time of radiation therapy.
Table 8. Risks of Hypothyroidism (Compensated or Uncompensated) After Radiation Therapy for Pediatric Malignancies, Grouped by Mean Thyroid Dose, Age, and Sexa Mean Thyroid Dose Risk of Hypothyroidismb Age <14 yc Age >15 yc Female Male Female Male a Adapted from Milano et al.[19] b Any hypothyroidism (i.e., compensated or uncompensated). c Age 14 to 15 y was used as a cutoff because the two studies that analyzed age used different cut-points. Presumably, the risks of hypothyroidism in patients irradiated at ages 14 to 15 y would be intermediate to those shown for ages <14 y and >15 y. 10 Gy 10% 6% 14% 8% 20 Gy 22% 13% 29% 17% 30 Gy 39% 23% 53% 31% 40 Gy 59% 35% 79% 47% - The PENTEC research consortium performed a systematic review of radiation-associated hypothyroidism.[20]
- Among seven cohorts (250 patients), the dose associated with a 50% risk (D50) of hypothyroidism was 39 Gy (95% CI, 34.1–53.2).
- The risk was 20% for children who received a mean dose of 22 Gy in 2-Gy fractions.
Clinical presentation
- Most children treated with radiation therapy who develop hypothyroidism do so within the first 2 to 5 years posttreatment, but new cases can occur later.
- Reports of thyroid dysfunction differ depending on the dose of radiation, the length of follow-up, and the biochemical criteria used to make the diagnosis.[21]
- The most frequently reported abnormalities include the following:
- Elevated TSH.
- Depressed T4.
- Elevated TSH and depressed T4.
- Central hypothyroidism results from radiation exposure of the hypothalamic pituitary axis; there is typically a low free T4 in conjunction with low TSH.
- Compensated hypothyroidism includes an elevated TSH with a normal T4 and is asymptomatic. The natural history is unclear, but most endocrinologists support treatment.
- Uncompensated hypothyroidism includes both an elevated TSH and a depressed T4.
- Thyroid hormone replacement is beneficial for correction of the metabolic abnormality, and has clinical benefits for cardiovascular, gastrointestinal, and neurocognitive function.
Hyperthyroidism
While less common than hypothyroidism, childhood cancer survivors also experience an increased risk of hyperthyroidism.[2,16,22,23]
Evidence (prevalence of and risk factors for hyperthyroidism):
- CCSS investigators evaluated the prevalence of thyroid disease among 1,791 childhood Hodgkin lymphoma survivors treated between 1970 and 1986 and followed for a median of 14 years.[16]
- Hyperthyroidism was reported by 5% of survivors, which was eightfold greater than the incidence reported by the controls.
- Radiation dose of 35 Gy or more to the thyroid was the only risk factor identified for hyperthyroidism.
- Another CCSS study evaluated the risk of hyperthyroidism in relation to incidental therapeutic radiation dose to the thyroid and pituitary glands.[22]
- Hyperthyroidism was self-reported by 179 survivors, with 148 cases diagnosed 5 or more years after cancer diagnosis.
- The cumulative proportion of survivors with hyperthyroidism by 30 years after cancer diagnosis was 2.5% (95% CI, 2.0%–2.9%).
- Thyroid radiation increased the risk of hyperthyroidism with evidence of a linear thyroid radiation dose-response over the dose range of 0 Gy to 63 Gy.
- Radiation to the pituitary gland and chemotherapy were not significantly associated with hyperthyroidism.
- Radiation-associated risk of hyperthyroidism remained elevated longer than 25 years after exposure.
Thyroid nodules
The clinical manifestation of thyroid neoplasia among childhood cancer survivors ranges from asymptomatic, small, solitary nodules to large, intrathoracic goiters that compress adjacent structures.
The following factors are linked to an increased risk of thyroid nodule development:
- Radiation dose, time from diagnosis, and female sex.
- Any radiation field that includes the thyroid is associated with an excess risk of thyroid neoplasms, which may be benign (usually adenomas) or malignant (most often differentiated papillary carcinoma).[2,16,24,25,26,27]
- A CCSS study that included survivors of Hodgkin lymphoma identified time from diagnosis, female sex, and radiation dose of 25 Gy or higher as significant risk factors for thyroid nodule development.[16]
- Based on a cohort of 3,254 2-year childhood cancer survivors treated before 1986 and monitored for 25 years, the risk of thyroid adenoma increased with the size of the radiation dose to the thyroid during childhood cancer treatment and plateaued at doses exceeding 10 Gy.[25]
- CCSS investigators performed a nested case-control study to evaluate the magnitude of risk for thyroid cancer over the therapeutic radiation dose range of pediatric cancers. The risk of thyroid cancer increased with radiation doses up to 20 Gy to 29 Gy (OR, 9.8; 95% CI, 3.2–34.8), but declined at doses higher than 30 Gy, consistent with a cell-killing effect.[27]
- Age at time of radiation therapy.
- Based on the same cohort of 3,254 2-year childhood cancer survivors, the risk of thyroid adenoma per unit of radiation dose to the thyroid was higher if radiation therapy had been delivered before age 5 years. The risk was also higher in individuals who were younger than 40 years at the time of the study.[25]
- Younger age at time of radiation therapy has also been linked to an excess risk of thyroid carcinoma.[24,25,26,27]
- Exposure to 131I-MIBG.
- During childhood and adolescence, there is an increased risk of developing thyroid nodules, and potentially thyroid cancer, in patients exposed to 131I-MIBG.
- Clinicians caring for survivors treated with 131I-MIBG should be aware of the risks of developing thyroid dysfunction, thyroid nodules, and thyroid cancer.[28]
- Chemotherapy.
- An increased risk of thyroid nodules and cancer has also been observed in association with chemotherapy, independent of radiation exposure.[2,24,25]
- In a pooled study of two cohorts of 16,757 survivors that included 187 patients with secondary thyroid cancer, treatments with alkylating agents, anthracyclines, or bleomycin were associated with a significantly increased risk of thyroid cancer in individuals not exposed to radiation therapy.[29]
- In the CCSS, the rate ratio of developing thyroid cancer was 2.5 (P < .01) in survivors not treated with thyroid radiation when compared with sibling controls.[2]
- Areas of active research include defining the precise role of exposure to chemotherapy and developing risk prediction models for thyroid cancer in childhood cancer survivors on the basis of demographic and treatment-related risk factors.[30]
Screening for thyroid cancer
- Several studies have demonstrated that ultrasonography is superior to clinical examination for detecting thyroid nodules and thyroid cancers, and they have characterized ultrasonographic features of nodules that are more likely to be malignant.[31,32,33]
- Primary screening for thyroid neoplasia (beyond physical examination with thyroid palpation) remains controversial because of the lack of data indicating a survival benefit and quality-of-life benefit associated with early detection and intervention.[34,35]
- Because these lesions tend to be indolent, are rarely life-threatening, and may clinically manifest many years after exposure to radiation, there are significant concerns regarding the costs and harms of overscreening.[36]
- Expert panels have refrained from specifically endorsing or discouraging the use of ultrasonography as a screening tool for thyroid cancer and this continues to be an active area of investigation.[37]
- Following a systematic assessment of the evidence, the International Guideline Harmonization Group concluded that initiation of surveillance and the type of surveillance modality (thyroid palpation vs. ultrasonography) should be determined by shared decision-making between the health care provider and survivor after carefully considering the benefits and harms. A decision aid to facilitate discussion accompanies their recommendations.[34]
For information about subsequent thyroid cancers, see the Subsequent Neoplasms section.
Posttransplant thyroid dysfunction
Survivors of pediatric hematopoietic stem cell transplant (HSCT) are at increased risk of thyroid dysfunction.[38,39]
- In a retrospective study of a single pediatric transplant unit, 244 pediatric patients were observed over a 20-year period. These patients had undergone HSCT for malignant or nonmalignant diseases between 1999 and 2018. Patients were assessed with a minimum of four thyroid function tests and one or more thyroid ultrasounds sequentially after HSCT.[39]
- Thyroid complications were detected in 19.7% of patients.
- The 15-year cumulative incidence of either autoimmune or nonautoimmune thyroid dysfunctions (34%) did not differ statistically between patients who received total-body irradiation (TBI)–based regimens and patients who received chemotherapy-based regimens (P = .23). The cumulative incidence after busulfan-based conditioning was similar to that of TBI (10-year cumulative incidence, 22.2% vs. 25.9%, respectively).
- The cumulative incidence of nonautoimmune hypothyroidism was statistically higher after busulfan-based conditioning (12.4%) than after other chemotherapy-only–based conditioning regimens (3.1%; P = .02, 5-year cumulative incidence).
- The overall incidence of thyroid nodules was low for the first 5 years after HSCT (1.9%) but increased steeply over time, with a 15-year cumulative incidence as high as 52.1%. Patients who received TBI-based conditioning regimens had a higher 15-year cumulative incidence of nodules (66.8%) than patients who received chemotherapy-only regimens (33.6%; P = .02).
- Age older than 10 years at transplant showed a protective effect (HR, 0.42).
- Sonographic follow-up showed a progressive statistically significant reduction in thyroid anteroposterior diameter among patients who received TBI-based conditioning regimens (P = .005) but not in those who received chemotherapy-only regimens.
- In a report from the Fred Hutchinson Cancer Research Center, the risk of thyroid dysfunction after HSCT was much lower (15%–16%) after fractionated TBI, as opposed to single-dose TBI (46%–48%).[38]
- The increased risk of thyroid dysfunction did not differ between children receiving a TBI-based or busulfan-based regimen (P = .48).
- Other high-dose therapies have not been studied.
TSH/TRH deficiency (central hypothyroidism) is discussed with late effects that affect the pituitary gland.
Table 9 summarizes thyroid late effects and the related health screenings.
| Predisposing Therapy | Endocrine/Metabolic Effects | Health Screening |
|---|---|---|
| 131I-MIBG = Iodine I 131-metaiodobenzylguanidine; T4 = thyroxine; TSH = thyroid-stimulating hormone. | ||
| a Adapted from theChildren's Oncology Group Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers. | ||
| Radiation exposing thyroid gland; thyroidectomy | Primary hypothyroidism | TSH level |
| Radiation exposing thyroid gland | Hyperthyroidism | Free T4 level |
| TSH level | ||
| Radiation exposing thyroid gland, including 131I-MIBG | Thyroid nodules | Thyroid examination |
| Thyroid ultrasonography | ||
Hypothalamus-Pituitary Axis
Survivors of childhood cancer are at risk of developing a spectrum of neuroendocrine abnormalities, primarily because of the effect of radiation therapy on the hypothalamus.
- There are two categories of childhood cancer survivors who experience hypothalamus-pituitary dysfunction after radiation—survivors with a CNS tumor and survivors treated for a non-CNS tumor of the head or neck or leukemia and/or individuals with a history of an HSCT.[40]
- In addition, tumor development or surgical resection close to the hypothalamus and/or pituitary gland may induce direct anatomical damage to these structures and result in hypothalamic-pituitary dysfunction.
- Essentially all of the hypothalamic-pituitary axes are at risk.[41,42,43]
The quality of the literature regarding pituitary endocrinopathy among childhood cancer survivors is often limited by retrospective data collection, small sample size, cohort selection and participation bias, heterogeneity in treatment approach, time since treatment, and method of ascertainment. However, the evidence linking this outcome with radiation therapy, surgery, and tumor infiltration is compelling because affected individuals typically present with metabolic and developmental abnormalities early in follow-up.
The risk of hypothalamus-pituitary dysfunction increases with higher doses of radiation therapy. When the radiation therapy dose exceeds 30 Gy, there is a higher risk of developing hypothalamus-pituitary disorders, including adrenocorticotropic hormone (ACTH) deficiency, luteinizing hormone (LH)/follicle-stimulating hormone (FSH) deficiency, and TSH deficiency.[40]
Central diabetes insipidus
Central diabetes insipidus may herald the diagnosis of craniopharyngioma, suprasellar germ cell tumor, or Langerhans cell histiocytosis.[44,45,46]
- Diabetes insipidus may occur as an isolated pituitary deficiency at presentation of sellar/suprasellar tumors, although additional pituitary hormone deficiencies may develop with tumor progression.
- More commonly, diabetes insipidus occurs in the context of panhypopituitarism caused by the effects of the tumor on the hypothalamic-pituitary-adrenal (HPA) axis, or as a consequence of surgical procedures undertaken for local tumor control.
- Central diabetes insipidus is unlikely to occur as a late effect from surgical tumor resection past 2 years of follow-up.[47] Its emergence past that time should prompt assessment for tumor changes or other causes.
- Central diabetes insipidus has not been reported as a late effect of cranial irradiation in childhood cancer survivors.[3]
Anterior pituitary hormone deficiency
Deficiencies of anterior pituitary hormones and major hypothalamic regulatory factors are common late effects among survivors treated with cranial irradiation.[43]
Evidence (prevalence of anterior pituitary hormone deficiency):
- Young patients with brain tumors are particularly vulnerable to hypothalamic-pituitary dysfunction. One study included 718 childhood brain tumor survivors who were monitored for a median of 7.9 years.[48]
- No differences were observed in the prevalence of hypothalamic-pituitary dysfunction among infants (0–1 years), toddlers (≥1–3 years), or older age groups at diagnosis, despite the fact that radiation therapy was less frequently used in infants.
- Radiation exposure (OR, 16.44; 95% CI, 8.93–30.27), suprasellar tumor location (OR, 44.76; 95% CI, 19.00–105.49), and younger age (OR, 1.11; 95% CI, 1.05–1.18) were associated with hypothalamic dysfunction.
- Infant and toddler brain tumor survivors showed more weight gain (P < .0001) and smaller height standard deviation score (SDS) (P = .001) during follow-up than survivors diagnosed at an older age.
- Among non-irradiated survivors, those who were infants and toddlers at diagnosis were significantly more frequently diagnosed with TSH, ACTH, and antidiuretic hormone (ADH) deficiency, compared with survivors diagnosed at an older age, presumably caused by systemic therapies or the trauma of neurosurgery.
- A study targeting more refined data on the radiation doses associated with pituitary insufficiency analyzed 102 patients treated for tumors that included radiation therapy exposures (CNS, head and neck, hematologic malignancies) between 2008 and 2019. The median (interquartile range [IQR]) age at radiation therapy was 9.0 years (6.0–12.0 years), and the median follow-up was 5.7 years (3.5–9.1 years). Most patients received focal brain radiation therapy (36.3%) or TBI (32.4%). The most frequent diagnoses were ALL (25.5%) and medulloblastoma (17.6%).[49]
- Most patients developed pituitary insufficiency (64 patients; 62.7%). Forty-one percent of patients had one hormone deficiency and 38% had two hormone deficiencies.
- Growth hormone deficiency (58 patients; 56.9%) and TSH deficiency (32 patients; 31.4%) were most common.
- Patients who developed pituitary insufficiency had received a higher maximum pituitary dose (median [IQR], 44.0 Gy [20.4–54.0] vs. 18.2 Gy [14.4–52.6]; P = .008). Doses of 40 to 49 Gy or higher than 50 Gy led to a higher cumulative incidence rate than doses lower than 20 Gy (HR, 4.07; P < .001 and HR, 3.04; P < .001, respectively).
- However, even at lower dose bands, levels of pituitary insufficiency were significant. The 5-year cumulative incidence was higher than 30% for growth hormone deficiency with doses lower than 20 Gy and for TSH deficiency with doses of 20 to 29 Gy.
- In a single-institution study, 1,713 adult survivors of childhood cancers and brain tumors (median age, 32 years) were monitored for a median follow-up of 25 years.[42]
- The prevalence of hypothalamic-pituitary axis disorders was 56.4% in individuals exposed to cranial radiation therapy at doses of 18 Gy or higher.
- A study of 3,141 childhood cancer survivors who were systematically evaluated for hypothalamic-pituitary disorders at a median follow-up of 24.1 years reported the following:[50]
- For patients who were treated with hypothalamic-pituitary radiation therapy (n = 1,089), the following was observed:
- The estimated prevalence of growth hormone deficiency was 40.2%.
- The estimated prevalence of TSH deficiency was 11.1%.
- The estimated prevalence of LH/FSH deficiency was 10.6%.
- The estimated prevalence of ACTH deficiency was 3.2%.
- The estimated prevalence of central precocious puberty was 0.9%.
- For patients who did not receive hypothalamic-pituitary radiation therapy, the estimated prevalence of growth hormone deficiency was 6.2% and less than 1% for the other hypothalamic-pituitary disorders.
- Clinical factors independently associated with hypothalamic-pituitary disorders included the following:
- Hypothalamic-pituitary radiation therapy (even at relatively low doses, except for ACTH deficiency which was not observed until >30 Gy).
- Alkylating agents (growth hormone deficiency, LH/FSH deficiency).
- Intrathecal chemotherapy (growth hormone deficiency).
- Hydrocephalus with shunt placement (growth hormone deficiency, LH/FSH deficiency).
- Seizures (TSH deficiency, ACTH deficiency).
- Stroke (growth hormone deficiency, TSH deficiency, LH/FSH deficiency, ACTH deficiency).
- Adverse outcomes associated with hypothalamic-pituitary disorders included the following:
- Short stature (growth hormone deficiency, TSH deficiency).
- Severe bone mineral deficit (growth hormone deficiency, LH/FSH deficiency).
- Obesity (LH/FSH deficiency).
- Frailty (growth hormone deficiency).
- Impaired physical health-related quality of life (TSH deficiency).
- Sexual dysfunction (LH/FSH deficiency).
- Impaired memory and processing speed (growth hormone deficiency, TSH deficiency).
- For patients who were treated with hypothalamic-pituitary radiation therapy (n = 1,089), the following was observed:
The International Late Effects of Childhood Cancer Guideline Harmonization Group (IGHG) consisting of 42 interdisciplinary international experts performed a systematic literature search on hypothalamic-pituitary axis surveillance in childhood cancer survivors.[40]
- They noted that hypothalamic-pituitary axis radiation exposure increased the risk for hypothalamic-pituitary dysfunction, with a dose dependent relationship. Doses of radiation therapy higher than 18 Gy are associated with a higher risk for growth hormone deficiency and central precocious puberty.
- Deficiencies in ACTH, TSH, and LH/FSH generally occur after doses higher than 30 Gy.
- The panel noted that childhood cancer survivors who have had local tissue injury to the hypothalamic-pituitary region are at risk of developing hypothalamic-pituitary dysfunction from the time of diagnosis or surgery for a brain tumor located near or within the hypothalamic-pituitary region or from occurrence of hydrocephalus (specifically at risk for growth hormone deficiency and central precocious puberty).
- Individuals exposed to radiation are at risk of developing hypothalamic-pituitary dysfunction one year from completion of radiation therapy.
- Childhood cancer survivors remain particularly at risk of growth hormone deficiency for at least 15 years after cancer diagnosis or treatment exposure. The risk beyond 15 years depends on individual patient factors. For central precocious puberty, patients remain at risk until age 8 years in girls and age 9 years for boys.
The six anterior pituitary hormones and their major hypothalamic regulatory factors are outlined in Table 10.
| Pituitary Hormone | Hypothalamic Factor | Hypothalamic Regulation of the Pituitary Hormone |
|---|---|---|
| (–) = inhibitory; (+) = stimulatory. | ||
| Growth hormone (GH) | GH-releasing hormone | + |
| Somatostatin | – | |
| Prolactin | Dopamine | – |
| Luteinizing hormone (LH) | Gonadotropin-releasing hormone | + |
| Follicle-stimulating hormone (FSH) | Gonadotropin-releasing hormone | + |
| Thyroid-stimulating hormone (TSH) | Thyroid-releasing hormone | + |
| Somatostatin | – | |
| Adrenocorticotropic hormone (ACTH) | Corticotropin-releasing hormone | + |
| Vasopressin | + | |
Growth hormone deficiency
Growth hormone deficiency is the most common and often the first anterior pituitary deficit to occur after cranial radiation therapy. In childhood survivors of CNS tumors, the overall prevalence of growth hormone deficiency is 12.5%.[3]
- The risk increases with radiation dose and time since treatment.
- Growth hormone deficiency can result from relatively low doses of cranial radiation.[51]
- Growth hormone deficiency can develop after 18 Gy to 24 Gy of cranial radiation, which is used to treat patients with ALL and lymphoma. The higher the radiation dose, the earlier that growth hormone deficiency will occur after treatment.[52]
- Approximately 60% to 80% of pediatric patients with brain tumors who received radiation therapy doses higher than 30 Gy will have impaired serum growth hormone response to provocative stimulation, usually within 5 years of treatment.[53,54]
Evidence (radiation-dose response relationship of growth hormone deficiency in childhood brain tumor survivors):
- In a report of 156 patients with medulloblastoma who were treated from 2003 to 2013 in the SJMB03 study, the following was observed:[55]
- The 5-year cumulative incidence of growth hormone deficiency was 68.9%, and the cumulative incidence of growth hormone replacement was 48.1%.
- Growth hormone deficiency was associated with increased hypothalamus dose (HR, 1.035; P = .0055) in average-risk patients and in high-risk patients who had a cerebrospinal fluid shunt (HR, 2.532; P = .0049).
- A study of conformal radiation therapy (CRT) in children with CNS tumors indicates that growth hormone insufficiency can usually be demonstrated within 12 months of radiation therapy, depending on hypothalamic dose-volume effects.[56]
- In a report featuring data from 118 patients with localized brain tumors who were treated with radiation therapy, peak growth hormone was modeled as an exponential function of time after CRT and mean radiation dose to the hypothalamus.[54]
- The average patient was predicted to develop growth hormone deficiency with the following combinations of time after CRT and mean dose to the hypothalamus: 12 months and more than 60 Gy; 36 months and 25 Gy to 30 Gy; and 60 months and 15 Gy to 20 Gy.
- A cumulative dose of 16.1 Gy to the hypothalamus would be considered the mean radiation dose causing a 50% risk of growth hormone deficiency at 5 years (TD50/5) (see Figure 7).
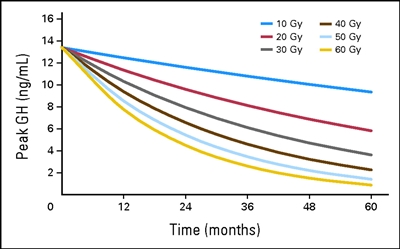
Figure 7. Peak growth hormone (GH) according to hypothalamic mean dose and time after start of radiation. According to equation 2, peak GH = exp{2.5947 + time × [0.0019 − (0.00079 × mean dose)]}. Thomas E. Merchant, Susan R. Rose, Christina Bosley, Shengjie Wu, Xiaoping Xiong, and Robert H. Lustig, Growth Hormone Secretion After Conformal Radiation Therapy in Pediatric Patients With Localized Brain Tumors, Journal of Clinical Oncology, volume 29, issue 36, pages 4776-4780. Reprinted with permission. © (2011) American Society of Clinical Oncology. All rights reserved. - A PENTEC review reported on the risk of growth hormone deficiency for childhood cancer survivors treated with radiation therapy.[20]
- The normal tissue complication probability modeling for growth hormone deficiency (18 cohorts, 545 patients) found that the D50 was 24.9 Gy (95% CI, 20.9–28.0).
- The normal tissue complication probability model fit for whole-brain irradiation in children with a median age of older than 5 years indicated a 20% risk of growth hormone deficiency for patients who received a mean dose of 21 Gy in 2-Gy fractions to the hypothalamic-pituitary axis.
Evidence (risk of growth deficits in childhood cancer survivors):
- One study evaluated 127 patients with ALL treated with 24 Gy, 18 Gy, or no cranial radiation therapy (treatment era, 1980s–1990s).[57]
- The change in height, compared with population norms expressed as the SDS, was significant for all three groups. The dose response was -0.49 ± 0.14 for the group that did not receive radiation therapy, -0.65 ± 0.15 for the group that received 18 Gy of radiation therapy, and -1.38 ± 0.16 for the group that received 24 Gy of radiation therapy.
- Survivors of childhood ALL who are treated with chemotherapy alone are also at increased risk for adult short stature, although the risk is highest for those treated with cranial and craniospinal radiation therapy at a young age.[58] In a cross-sectional study, attained adult height was determined for 2,434 ALL survivors participating in the CCSS.
- All survivor treatment exposure groups (chemotherapy alone and chemotherapy with cranial or craniospinal radiation therapy) had decreased adult height and an increased risk of adult short stature (height SDS < -2), compared with siblings (P < .001).
- Compared with siblings, the risk of short stature for survivors treated with chemotherapy alone was elevated (OR, 3.4; 95% CI, 1.9–6.0).
- Among survivors, significant risk factors for short stature included diagnosis of ALL before puberty, higher-dose cranial radiation therapy (≥20 Gy vs. <20 Gy), any radiation therapy to the spine (which effects vertebral bodies), and female sex.
- The impact of chemotherapy alone on growth in 67 survivors treated with contemporary regimens for ALL was statistically significant at -0.59 SD. The loss of growth potential did not correlate with growth hormone status in this study, further highlighting the participation of other factors in the growth impairments observed in this population.[59]
- In a longitudinal study of 372 survivors of ALL who were treated on a single-institution chemotherapy-only trial, the following were observed:[60]
- Height z-scores declined during treatment and improved after therapy.
- Younger age at diagnosis (2 to <10 years), low-risk ALL status, white blood cell count below 50 × 109 /L at diagnosis, or CNS-negative status were associated with significant improvements in z-scores for height during the off-therapy period compared with those older at diagnosis (age ≥10 years), those with standard-risk/high-risk ALL status, those with a white blood cell count of 50 × 109 /L or higher, or CNS-positive status.
- The loss in height potential in older patients was attributed to attenuation of the growth spurt during treatment without improvement after therapy and to chemotherapy intensity in patients with standard- or high-risk disease features.
- A French CCSS study evaluated risk factors for short adult height and growth hormone deficiency in 2,965 childhood cancer survivors using clinical and treatment data available in medical records. Patients treated with growth hormones (6.4%) were excluded.[61]
- Independent risk factors for short adult height included being young at the time of cancer treatment (RR, 0.9 per year of age), having a short height at diagnosis (≤2 SDS: RR, 6.7), and having received treatment with pituitary radiation (5–20 Gy: RR, 4.2; 20–40 Gy: RR, 10.2; ≥40 Gy: RR, 19.5), busulfan (RR, 4.5), or more than 300 mg/m2 of lomustine (300–600 mg/m2: RR, 4.2 and ≥600 mg/m2: RR, 9.1).
- Children who were treated with 15 Gy or higher of radiation to 90% or more volume of seven or more vertebrae without pituitary irradiation had an increased risk of short adult stature (RR, 4.6). This risk increased by 1.3-fold to 2.4-fold if they also received pituitary radiation therapy.
- A St. Jude Children's Research Hospital investigation evaluated long-term (median follow-up, 10.2 years) height outcomes among 212 pediatric patients with CNS embryonal tumors who were treated with CSI at 23.4 Gy (n = 147) or 36 Gy or higher (n = 65).[62]
- Compared with U.S. standards, mean final height z-scores at age 18 years were -1.3 for female and -1.5 for male survivors.
- Factors associated with risk of height impairment included younger age at the time of CSI, higher CSI dose, and female sex.
- Factors associated with higher growth rates before the age of 15 years included older age at CSI, male sex, CSI dose lower than 36 Gy, replacement therapy for growth hormone and central adrenal insufficiency, and White race.
Growth after hematopoietic stem cell transplant (HSCT)
- Children who undergo HSCT with TBI have a significant risk of both growth hormone deficiency and the direct effects of radiation on skeletal development.[63,64,65]
- The risk of growth hormone deficiency is increased with single-dose TBI as opposed to fractionated TBI, pretransplant cranial irradiation, female sex, and posttreatment complications such as graft-versus-host disease (GVHD).[63,64,65]
- Hyperfractionation of the TBI dose markedly reduces risk in patients who have not undergone cranial irradiation for CNS leukemia prophylaxis or therapy.[66]
- Regimens containing busulfan and cyclophosphamide appear to increase risk in some studies,[65,67] but not others.[68]
Evidence (growth hormone deficiency in childhood HSCT survivors):
- The late effects that occur after HSCT have been studied by the Late Effects Working Party of the European Group for Blood and Marrow Transplantation. Among 181 patients with aplastic anemia, leukemias, and lymphomas who underwent HSCT before puberty, the following results were observed:[69,70]
- An overall decrease in final height–SDS value was found, compared with height at transplant and genetic height. The mean loss of height is estimated to be approximately 1 height–SDS (6 cm), compared with the mean height at time of HSCT and mean genetic height.
- The type of transplant, GVHD, and growth hormone or steroid treatment did not influence final height.
- TBI (single-dose more than fractionated-dose radiation therapy), male sex, and young age at transplant were found to be major factors for long-term height loss.
- Most patients (140 of 181) reached adult height within the normal range of the general population.
- Growth hormone deficiency has been reported after lower doses with a single fraction of 10 Gy and fractionated doses of 12 to 18 Gy of TBI.[71]
Growth hormone replacement therapy
- Growth hormone replacement therapy provides the benefit of optimizing height outcomes among children who have not reached skeletal maturity.[43] The diagnosis requires specialized dynamic testing.[43,72]
- Treatment with recombinant growth hormone (rGH) replacement therapy is generally delayed until 12 months after successful completion of cancer or brain tumor treatments and after a multidisciplinary discussion involving the prescribing pediatric endocrinologist, the primary oncologist, and other providers selected by the patient or family.[73]
- Safety concerns pertaining to the use of rGH in childhood cancer survivors have primarily been related to the mitogenic potential of the growth hormone stimulating tumor growth in a population with an increased risk of second neoplasms.[74] Most studies that report these outcomes, however, are limited by selection bias and small sample size.
Evidence (subsequent neoplasm risk after growth hormone deficiency replacement therapy):
- One study evaluated 361 growth hormone–treated cancer survivors enrolled in the CCSS and compared risk of recurrence, risk of subsequent neoplasm, and risk of death among survivors who did and did not receive treatment with growth hormone.[75]
- The RR of disease recurrence was 0.83 (95% CI, 0.37–1.86) for growth hormone–treated survivors.
- Growth hormone–treated participants were diagnosed with 15 subsequent neoplasms, all solid tumors, for an overall RR of 3.21 (95% CI, 1.88–5.46). This was mainly due to a small excess number of subsequent neoplasms observed in survivors of acute leukemia.[75]
- With prolonged follow-up, the elevation of subsequent cancer risk resulting from growth hormone diminished.[76]
- Compared with survivors not treated with growth hormone, those who were treated had a twofold excess risk of developing a subsequent neoplasm (RR, 2.15; 95% CI, 1.33–3.47; P < .002). Meningiomas were the most commonly observed neoplasms (9 of 20 tumors).[75]
- A study from the CCSS reported on the risk of subsequent CNS neoplasms after a longer period of follow-up.[77]
- The adjusted rate ratio of meningioma and gliomas in growth hormone–treated survivors of CNS tumors was 1.0 (95% CI, 0.6–1.8; P = .94), when compared with CNS tumor survivors who were not treated with growth hormone. This finding indicates negligible differences between the two groups for this particular risk.
- A review of existing data suggests that treatment with growth hormone is not associated with an increased risk of CNS tumor progression or recurrence, or new or recurrent leukemia.[78]
In general, the data addressing subsequent malignancies among childhood cancer survivors treated with growth hormone therapy should be interpreted with caution given the small number of events.[43,56,73,74,75,79,80]
As outlined in a consensus statement by the Growth Hormone Research Society, areas of uncertainty include the safety of growth hormone in children with cancer-predisposing conditions, its use in growth hormone–deficient children who are receiving maintenance therapy, and the overall benefit-risk ratio in adult survivors.[81]
Disorders of LH and FSH
- Pubertal development can be adversely affected by cranial radiation therapy.
- Doses higher than 18 Gy can result in central precocious puberty, while doses higher than 30 Gy to 40 Gy may result in LH/FSH deficiency.[50]
Central precocious puberty
Prevalence and risk factors
- Central precocious puberty is among the most common hypothalamic-pituitary dysfunctions. The prevalence varies across studies because of study cohort composition and method of ascertainment.[3,82,83]
- In the SJMB03 study, 156 children and adolescents with medulloblastoma were treated with surgery, risk-adapted photon craniospinal irradiation, and dose-intensive chemotherapy.[55]
- The 5-year cumulative incidence of precocious puberty was 2.0%.
- Children with CNS tumors within or near the hypothalamic-pituitary axis (including those with neurofibromatosis type 1) or those treated with cranial radiation are most vulnerable.[3]
- In a study of 178 childhood brain tumor survivors (median follow-up, 6.6 years), precocious puberty developed in 12.2% of survivors, with a 5-year cumulative incidence of 4.0%.[3]
- Central precocious puberty has been reported in children receiving cranial irradiation in doses of 18 Gy or higher.[82,84,85]
- Hydrocephalus also increases the risk of central precocious puberty.[86]
Diagnosis
- Central precocious puberty is defined by the onset of pubertal development before age 8 years in girls and 9 years in boys as a result of the premature activation of the hypothalamic-pituitary-gonadal axis.
- Assessment of puberty cannot be performed using testicular volume measurements in boys exposed to chemotherapy or direct radiation to the testes, given the toxic effect of these treatments on germ cells and repercussions on gonadal size.[87]
- The staging of puberty in males within this population relies on the presence of other signs of virilization, such as the presence of pubic hair and the measurement of morning plasma testosterone and LH levels.[87]
Treatment and outcomes associated with central precocious puberty
- Aside from the adjustment and psychosocial challenges associated with early pubertal development, precocious puberty can lead to the rapid closure of the skeletal growth plates and short stature. This deleterious effect can be further potentiated by growth hormone deficiency.[82,87]
- The increased growth velocity induced by pubertal development can mask concurrent growth hormone deficiency with seemingly normal growth velocity; this occurrence may mislead care providers.[87]
- The impact of central precocious puberty on linear growth can be ascertained by assessing the degree of skeletal maturation (or bone age) using an x-ray of the left hand.[88]
- Delaying the progression of puberty relies on the use of various gonadotropin-releasing hormone agonist preparations. This approach has been shown to improve growth prospects, especially when other pituitary abnormalities, including growth hormone deficiency, are concurrently treated.[43,89]
LH/FSH deficiency
- LH/FSH deficiency (also referred to as hypogonadotropic hypogonadism) can manifest through pubertal delay (after age 13 years in girls and 14 years in boys), arrested puberty, or symptoms of decreased sex hormone production, depending on age and pubertal status at the time of diagnosis.
- The risk of LH/FSH deficiency is highest among patients treated with cranial radiation at doses greater than or equal to 30 Gy. LH/FSH deficiency following the exposure to lower doses can occur at delayed time points.[4]
- With higher doses of cranial radiation therapy (>35 Gy), deficiencies in LH/FSH can be seen, with a cumulative incidence of 10% to 20% at 5 to 10 years posttreatment.[4,86]
- The treatment of LH/FSH deficiency relies on sex-hormone replacement therapy adjusted to age and pubertal status.[43]
TSH/TRH deficiency
TSH deficiency (also referred to as central hypothyroidism) in survivors of childhood cancer can have profound clinical consequences and be underappreciated. Among survivors of head and neck tumors treated with radiation therapy potentially exposing the hypothalamic-pituitary region and the thyroid gland, hypothyroidism may result from TRH and/or TSH deficiency (central hypothyroidism), thyroid gland dysfunction (primary hypothyroidism), or a combination of central and primary causes.
Prevalence and risk factors
- The risk of TSH deficiency is highest among patients treated with cranial radiation at doses of 30 Gy or higher. TSH deficiency following the exposure to lower doses can occur at delayed time points.[4]
- The cumulative incidence of TSH deficiency was 23% (± 8%) among embryonal brain tumor survivors treated with risk-adapted CSI, conformal primary site irradiation, and high-dose chemotherapy. Radiation dose to the hypothalamus in excess of 42 Gy is associated with an increased risk of developing TSH deficiency (44% ± 19% for a dose of ≥42 Gy and 11% ± 8% for a dose of <42 Gy).[90]
- In a report of 156 children and adolescents with medulloblastoma who were treated with surgery, risk-adapted photon craniospinal irradiation, and dose-intensive chemotherapy between 2003 and 2013, the incidence of hypothyroidism was 48.4%.[55]
- In average-risk patients, hypothyroidism was associated with younger age (HR, 0.902; P = .0070), hypothalamus dose (HR, 1.039; P = .0273), and thyroid dose (HR, 1.070; P = .0263). The mean radiation therapy dose was 34.8 Gy (standard deviation [SD], 7.5) to the hypothalamus and 17.4 Gy (SD, 5.4) to the thyroid.
- In high-risk patients, hypothyroidism was associated with increased hypothalamus dose (HR, 1.068; P = .0671) and thyroid dose (HR, 1.050; P = .0515). The mean radiation therapy dose was 47.8 Gy (SD, 4.87) to the hypothalamus and 25.8 Gy (SD, 7.2) to the thyroid.
- The investigators were not able to reliably distinguish between central and primary hypothyroidism, but they estimated that 8 of 85 patients were initially diagnosed with central hypothyroidism.
- Among medulloblastoma survivors treated with photon (median follow-up, 9.6 years) or proton (median follow-up, 3.8 years) radiation therapy, primary hypothyroidism developed in 12 of 54 patients (22%) after photon radiation therapy and 3 of 41 patients (7%) after proton radiation therapy (HR, 2.1; P = .27). Central hypothyroidism (TSH deficiency) developed in 13 of 54 patients (24%) after photon radiation therapy and 4 of 41 patients (10%) after proton radiation therapy (HR, 2.16, P = .18).[91]
- Among 118 medulloblastoma survivors (median follow-up, 5.6 years), the estimated cumulative incidence of hypothyroidism was 35.8% (95% CI, 26.7%–47.1%) by 5 years after radiation therapy.[18]
- The median time from the end of radiation therapy to the development of hypothyroidism was 2.1 years (range, 0.1–7.1 years) after proton radiation therapy and 2.9 years (range, 0.8–7.2 years) after photon radiation therapy.
- The rate of hypothyroidism (HR, 2.36; 95% CI, 1.11–5.02) was higher in patients treated with photon radiation therapy than in those treated with proton radiation therapy.
- Differences in hypothyroidism risk by radiation modality were largely attributed to higher rates of primary hypothyroidism after photon radiation therapy (HR, 4.61; 95% CI, 1.20–17.66).
- Patients with central hypothyroidism should undergo testing for other hypothalamic-pituitary deficiencies before thyroid replacement. Thyroid replacement can enhance the clearance of cortisol, which exacerbates any underlying adrenal insufficiency and contributes to the possibility of adrenal crisis.
- In a study of 189 children and young adults (aged <26 years) with brain tumors who were treated with proton radiation therapy, the 4-year actuarial rate of hypothyroidism was 20.1%. Ninety percent of the cases were related to central TSH deficiency.[17]
Clinical presentation and diagnosis
- Symptoms of central hypothyroidism (e.g., asthenia, edema, drowsiness, and skin dryness) may have a gradual onset and go unrecognized until thyroid replacement therapy is initiated.
- In addition to delayed puberty and slow growth, hypothyroidism may cause fatigue, dry skin, constipation, increased sleep requirement, and cold intolerance.
- Individuals with TSH deficiency usually have low plasma free T4 levels and either low or inappropriately normal TSH levels. Declining free T4 levels within the normal range may also be predictive of TSH deficiency. Clinicians should not hesitate to reassess survivors with this pattern of thyroid function, especially in the presence of symptoms of hypothyroidism.[92]
- Mixed primary and central hypothyroidism can also occur because of separate injuries to the thyroid gland and the hypothalamus (e.g., radiation injury to both structures), leading to mildly elevated TSH values despite the contribution of hypothalamic-pituitary deficits to hypothyroidism in affected individuals.
Management of TSH deficiency
- Thyroid hormone replacement therapy using levothyroxine represents the mainstay of treatment of TSH deficiency.
- The dose of levothyroxine needs to be adjusted solely using plasma free T4 levels. The levels of TSH are expected to remain low during therapy, given the central nature of this deficiency.
- Central hypothyroidism should not be treated before assessment of the functioning of other hypothalamic-pituitary deficiencies, because it could precipitate an adrenal crisis in patients with ACTH deficiency.
ACTH deficiency
Prevalence and risk factors
- ACTH deficiency is less common than other neuroendocrine deficits but should be suspected in patients who have a history of brain tumors (regardless of therapy modality), cranial radiation therapy, growth hormone deficiency, or central hypothyroidism.[43,90,93,94]
- ACTH deficiency develops almost exclusively in survivors previously exposed to hypothalamic-pituitary doses of 30 Gy or greater.
- The cumulative incidence of ACTH deficiency was 38% (± 6%) among embryonal brain tumor survivors treated with risk-adapted CSI, conformal primary site irradiation, and high-dose chemotherapy. ACTH status was not affected by the dose of radiation therapy administered to the hypothalamus (median, 42.2 Gy for no ACTH deficiency vs. 41.3 Gy for ACTH deficiency).[90]
- In a study of 189 children and young adults (aged <26 years) with brain tumors who were treated with proton radiation therapy, the 5-year actuarial rate of ACTH deficiency was 8%, occurring almost exclusively after ≥40 Gy to the hypothalamus and pituitary.[17]
- One report included 156 children and adolescents with medulloblastoma who were treated with surgery, risk-adapted photon craniospinal irradiation, and dose-intensive chemotherapy in the SJMB03 study. The 5-year cumulative incidence of adrenal insufficiency was 13.0%.[55] Adrenal insufficiency was associated with increased hypothalamus dose (HR, 1.112; P < .0001).
- Although uncommon, ACTH deficiency can occur in patients treated with intracranial radiation doses of less than 24 Gy and in patients with non-CNS tumors or hematological malignancies distant from the hypothalamic-pituitary region. The use of glucocorticoid therapy in treatment protocols may also be associated with steroid-induced adrenal insufficiency, which in some cases may be prolonged.[95,96,97]
- In a PENTEC report on ACTH deficiency (6 cohorts, 230 patients), the dose associated with a 50% risk was 61 Gy (95% CI, 44.7–119.4).[20] The risk of ACTH deficiency was 20% in children who received a mean dose of 34 Gy in 2-Gy fractions to the hypothalamus-pituitary axis.
Diagnosis and management
- The diagnosis of ACTH deficiency should be suspected when low plasma levels of morning cortisol are measured (a screening cortisol level collected at 8 AM that is 10 µg/dL or more is reassuring for ACTH sufficiency, whereas a value of 5 µg/dL or lower is suspicious for insufficiency).
- Confirmation is necessary using dynamic testing such as the low-dose ACTH stimulation test.[93]
- Because of the substantial risk of central adrenal insufficiency among survivors treated with cranial radiation doses exceeding 30 Gy to the hypothalamic-pituitary axis, endocrine monitoring with periodic dynamic testing as clinically indicated is recommended for this high-risk group.[43]
- Patients with partial ACTH deficiency may have only subtle symptoms unless they become ill.[43]
- Illness can disrupt these patients' usual homeostasis and cause a more severe, prolonged, or complicated course than expected. As in complete ACTH deficiency, incomplete or unrecognized ACTH deficiency can be life-threatening during concurrent illness.
- The treatment of ACTH deficiency relies on replacement with hydrocortisone, including stress dosing in situations of illness to adjust to the body's physiologically increased need for glucocorticoids.[43]
Hyperprolactinemia
- Hyperprolactinemia has been described in patients who received radiation therapy to the hypothalamus in doses higher than 50 Gy or who underwent surgery that disrupted the integrity of the pituitary stalk.[98]
- Primary hypothyroidism may lead to hyperprolactinemia as a result of hyperplasia of thyrotrophs and lactotrophs, presumably caused by TRH hypersecretion.
- The prolactin response to TRH is usually exaggerated in these patients.[51,99]
- Hyperprolactinemia may result in delayed puberty, galactorrhea, menstrual irregularities, loss of libido, hot flashes, infertility, and osteopenia. Hyperprolactinemia resulting from cranial radiation therapy is rarely symptomatic and is frequently associated with hypogonadism (both central and primary).
- Hyperprolactinemia rarely requires treatment.[100]
Table 11 summarizes pituitary gland late effects and the related health screenings.
| Predisposing Therapy | Endocrine/Metabolic Effects | Health Screening |
|---|---|---|
| BMI = body mass index; FSH = follicle-stimulating hormone; LH = luteinizing hormone; T4 = thyroxine; TSH = thyroid-stimulating hormone. | ||
| a Adapted from theChildren's Oncology Group Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers. | ||
| b Testicular volume measurements are not reliable in the assessment of pubertal development in boys exposed to chemotherapy or direct radiation to the testes. | ||
| c Appropriate only at diagnosis. TSH levels are not useful for follow-up during replacement therapy. | ||
| Tumor or surgery affecting hypothalamus/pituitary. Radiation exposing hypothalamic-pituitary axis. | Growth hormone deficiency | Assessment of nutritional status |
| Height, weight, BMI, Tanner stageb | ||
| Tumor or surgery affecting hypothalamus/pituitary or optic pathways; hydrocephalus. Radiation exposing hypothalamic-pituitary axis. | Precocious puberty | Height, weight, BMI, Tanner stageb |
| FSH, LH, estradiol, or testosterone levels | ||
| Tumor or surgery affecting hypothalamus/pituitary. Radiation exposing hypothalamic-pituitary axis. | Gonadotropin deficiency | History: puberty, sexual function |
| Examination: Tanner stageb | ||
| FSH, LH, estradiol or testosterone levels | ||
| Tumor or surgery affecting hypothalamus/pituitary. Radiation exposing hypothalamic-pituitary axis. | Central adrenal insufficiency | History: failure to thrive, anorexia, episodic dehydration, hypoglycemia, lethargy, unexplained hypotension |
| Endocrine consultation for those with radiation dose ≥30 Gy | ||
| Radiation exposing hypothalamic-pituitary axis. | Hyperprolactinemia | History/examination: galactorrhea |
| Prolactin level | ||
| Radiation exposing hypothalamic-pituitary axis. | Overweight/obesity | Height, weight, BMI |
| Blood pressure test | ||
| Components of metabolic syndrome (abdominal obesity, hypertension, dyslipidemia, impaired glucose metabolism) | Fasting blood glucose level and lipid profile | |
| Tumor or surgery affecting hypothalamus/pituitary. Radiation exposing hypothalamic-pituitary axis. | Central hypothyroidism | TSHc free thyroxine (free T4) level |
Testis and Ovary
Testicular and ovarian hormonal functions are discussed in the Late Effects of the Reproductive System section of this summary.
Metabolic Syndrome
An increased risk of metabolic syndrome or its components has been observed among survivors of childhood cancer. The evidence for this outcome ranges from clinically manifested conditions that are self-reported by survivors to retrospectively assessed data in medical records and hospital registries to systematic clinical evaluations of clinically well-characterized cohorts. Studies have been limited by cohort selection and participation bias, heterogeneity in treatment approach, time since treatment, and method of ascertainment. Despite these limitations, compelling evidence indicates that metabolic syndrome is highly associated with cardiovascular events and mortality.
Definitions of metabolic syndrome are evolving but generally include a combination of central (abdominal) obesity with at least two of the following features:[101]
- Hypertension.
- Atherogenic dyslipidemia (elevated triglycerides, reduced high-density lipoprotein [HDL] cholesterol).
- Abnormal glucose metabolism (fasting hyperglycemia, hyperinsulinism, insulin resistance, diabetes mellitus type 2).
Evidence (prevalence of and risk factors for metabolic syndrome in childhood cancer survivors):
- Investigators assessed the prevalence and determinants of metabolic syndrome in the Dutch Childhood Cancer Survivors Study (DCCSS) LATER 2 cohort. A total of 2,338 adult survivors of childhood cancer were assessed and compared with 132,226 adults from the Lifelines cohort. These individuals did not have histories of cancer.[102]
- Survivors showed a twofold increased risk of metabolic syndrome when compared with adults who did not have histories of cancer. This increased risk was mostly derived from an increased risk of dyslipidemia (increased triglycerides and/or low HDL-C levels).
- A high prevalence of metabolic syndrome (19.1%) was identified in this young survivor cohort (median age, 34.7 years).
- Other factors associated with metabolic syndrome were smoking (OR, 1.46), reduced physical activity (OR, 1.48), abdominal radiation therapy (OR, 2.13; >30 Gy), cranial radiation therapy (OR for 1–25 Gy, 2.89; OR for >25 Gy, 2.44), total-body irradiation (OR, 6.17), and underlying central nervous system tumor (OR, 1.78).
- French investigators evaluated the overall and age-specific prevalence of and risk factors for metabolic syndrome and its components among 650 adult survivors of childhood leukemia treated without HSCT.[103]
- The overall prevalence of the condition was 6.9%, with the following age-specific cumulative prevalence:
- 20 years—1.3%.
- 25 years—6.1%.
- 30 years—10.8%.
- 35 years—22.4%.
- The prevalence of individual components of the metabolic syndrome was as follows:
- Increased fasting glucose—5.8%.
- Increased triglycerides—11.7%.
- Increased abdominal circumference—16.7%.
- Decreased HDL cholesterol—26.8%.
- Increased blood pressure—36.7%.
- Clinical factors significantly predicting the risk of metabolic syndrome included male sex (OR, 2.64; 95% CI, 1.32–5.29), age at last evaluation (OR, 1.10; 95% CI, 1.04–1.17) and body mass index (BMI) at diagnosis (OR, 1.15; 95% CI, 1.01–1.32), but not cumulative steroid dose. Irradiated and nonirradiated patients exhibited different patterns of metabolic abnormalities, with more frequent abdominal obesity in irradiated patients and more frequent hypertension in nonirradiated patients.
- The overall prevalence of the condition was 6.9%, with the following age-specific cumulative prevalence:
- A study monitored 784 long-term childhood ALL survivors (median age, 31.7 years) for a median follow-up of 26.1 years.[104]
- The prevalence of metabolic syndrome was 33.6%, which was significantly higher than that in a cohort of age-, sex-, and race-matched controls (n = 777) from the National Health and Nutrition Examination Survey (RR, 1.43; 95% CI, 1.22–1.69).
- Risk factors associated with metabolic syndrome in this study included older age and past exposures to cranial radiation therapy.
- Components of the metabolic syndrome that were significantly more prevalent in ALL survivors than in controls included obesity, insulin resistance, hypertension, and decreased HDL levels.
- The French childhood leukemia survivors' cohort showed that the prevalence of metabolic syndrome was increased among childhood leukemia survivors (n = 1,025), relative to controls (n = 3,202).[105]
- Metabolic syndrome was found in 10.3% of patients (mean follow-up, 16.3 years) and 4.5% of controls (OR, 2.49; P < .001). Transplant patients treated with TBI had the highest risk (OR, 6.26; P < .001). Other treatment groups that also showed a higher risk than controls included patients treated with chemotherapy only. ORs were 1.68 (P = .005) after chemotherapy only, 2.32 (P = .002) after chemotherapy and cranial irradiation, and 2.18 (P = .057) after transplant without irradiation.
- Compared with controls, unique profiles were seen in survivors according to treatment. Patients who received TBI and developed metabolic syndrome had a smaller waist circumference than controls. In contrast, patients who were treated with cranial irradiation and developed metabolic syndrome had a larger waist circumference than controls. Additionally, TBI recipients had increased triglyceride levels, fasting glucose levels, and systolic blood pressure.
- In a prospective study of 164 long-term survivors of embryonal tumors treated with abdominal radiation therapy (median follow-up, 26 years), nephroblastoma (OR, 5.2) and neuroblastoma (OR, 6.5) survivors had more components of metabolic syndrome than did controls.[106]
- Compared with survivors who did not receive radiation therapy, survivors treated with abdominal irradiation had higher blood pressure, triglycerides, low-density lipoprotein cholesterol, and total fat percentage, which were assessed by dual-energy x-ray absorptiometry.
Lifestyle impact on modifiable risk factors
- Modifiable risk factors (such as diet, physical activity, and smoking habits) may impact the risk of developing metabolic syndrome in childhood cancer survivors.
- Several studies have provided support for the potential benefits of lifestyle modifications in reducing cardiovascular disease risk.[107,108,109]
Evidence (lifestyle modifications to reduce cardiovascular risk in childhood cancer survivors):
- Survivors participating in the SJLIFE study who were adherent to a heart-healthy lifestyle had a lower risk of metabolic syndrome.[107]
- Females (RR, 2.4; 95% CI, 1.7–3.3) and males (RR, 2.2; 95% CI, 1.6–3.0) in the cohort who did not follow recommended dietary and physical activity guidelines had a more than twofold excess risk of having clinical features of the metabolic syndrome.
- A CCSS investigation evaluated the impact of exercise on cardiovascular disease risk among survivors of Hodgkin lymphoma.[108]
- Vigorous exercise was associated with a lower risk of cardiovascular events in a dose-dependent manner, independent of cardiovascular risk profile and treatment.
- Survivors who were adherent to national vigorous-intensity exercise guidelines had a 51% reduction in the risk of any cardiovascular event compared with those not meeting the guidelines.
- Another CCSS investigation evaluated the association of exercise with mortality in adult survivors of childhood cancer.[109]
- After adjusting for chronic health conditions and treatment exposures, all-cause mortality was inversely associated with survivor-reported exercise quartiles (0, 3–6, 9–12, and 15–21 metabolic equivalent task [MET] hours/week).
- Survivors who endorsed recommended levels of vigorous exercise (≥9 MET hours/week) in early adulthood and those who increased exercise over 8 years had a lower risk of mortality.
Abnormal glucose metabolism
For individuals treated at a young age (age <11 years), abdominal radiation therapy and TBI are increasingly recognized as independent risk factors for diabetes mellitus in childhood cancer survivors.[2,110,111,112,113,114]
Evidence (risk factors for diabetes mellitus in childhood cancer survivors):
- A single-center cohort study of 532 long-term adult survivors (median follow-up, 17.9 years; median age, 25.6 years) observed the following:[111]
- Treatment, but not genetic variation, was strongly associated with the occurrence of the components of metabolic syndrome.
- Metabolic syndrome was more frequent in survivors who received cranial (23.3%, P = .002) or abdominal (23.4%, P = .009) radiation therapy than in survivors who did not receive radiation therapy (10.0%).
- A cross-sectional study evaluated cardiovascular risk factors and insulin resistance in a clinically heterogeneous cohort of 319 childhood cancer survivors 5 or more years since diagnosis and 208 sibling controls.[115]
- Insulin resistance was significantly higher in survivors treated with cisplatin plus cranial irradiation (92% brain tumors) and in those who received steroids but no cisplatin (most leukemia survivors), compared with siblings.
- Insulin resistance did not differ between survivors treated with surgery alone and siblings.
- Among survivors, analysis of individual chemotherapy agents failed to find associations with cardiovascular risk factors or insulin resistance.
- Compared with siblings, nearly all chemotherapeutic agents, when examined individually, seemed to be associated with a high cardiovascular risk profile, characterized by lower total lean body mass, higher percentage fat mass, and insulin resistance.
- In a European multicenter cohort of 2,520 childhood cancer survivors (median follow-up, 28 years), significant associations were found between diabetes mellitus and increasing doses of radiation therapy to the tail of the pancreas. This finding supports the contribution of radiation-induced islet cell injury to impairments of glucose homeostasis in this population.[112]
- A report from the CCSS compared 8,599 childhood cancer survivors with 2,936 randomly selected sibling controls, and adjusted for age, BMI, and several demographic factors.[116]
- The risk of diabetes mellitus was 1.8 times higher in survivors (95% CI, 1.3–2.5; P < .001).
- Significant associations were found between diabetes mellitus and young age at diagnosis (0–4 years), the use of alkylating agents, and abdominal radiation therapy or TBI.
- Survivors exposed to abdominal radiation had a 3.4-fold higher increased risk of diabetes (95% CI, 2.3–5.0; P < .001) when compared with siblings and after adjusting for BMI. Compared with siblings, survivors of neuroblastoma and Wilms tumor who were treated with abdominal radiation therapy had a 6.9-fold and 2.1-fold increased risk of diabetes, respectively. Individuals in these groups who had not been exposed to abdominal radiation therapy were not at increased risk.
- Survivors were significantly more likely to be receiving medication for hypertension, dyslipidemia, and/or diabetes mellitus than were sibling controls.
Table 12 summarizes metabolic syndrome late effects and the related health screenings.
| Predisposing Therapy | Potential Late Effects | Health Screening |
|---|---|---|
| BMI = body mass index. | ||
| a Adapted from theChildren's Oncology Group Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers. | ||
| Abdominal irradiation; total-body irradiation. | Components of metabolic syndrome (abdominal obesity, hypertension, dyslipidemia, impaired glucose metabolism) | Height, weight, BMI, blood pressure test |
| Laboratory tests: Fasting glucose and lipids | ||
Body Composition: Underweight, Overweight, and Obesity
- Childhood cancer survivors are at risk of experiencing abnormal body composition, which includes becoming underweight (BMI, <18.5), becoming overweight (BMI, >25.0 to BMI, <30.0), or being affected by obesity (BMI, ≥30.0).
- BMI at diagnosis has been identified as a significant predictor of being underweight or overweight at follow-up. This finding suggests that genetic or environmental factors contribute to the development or persistence of abnormal body composition.[117,118]
Underweight
- Approximately one of ten adult survivors of childhood cancer is underweight. CCSS investigators found that childhood cancer survivors who are underweight have an increased risk of late mortality.[119]
- Of the 9,454 survivors (median age, 35 years; an average of 17.5 years from diagnosis), 627 (6.6%) were underweight at the baseline survey or at the follow-up questionnaire. Of the 184 deaths, 29 were initially underweight at baseline.
- Underweight status was more common among females (9.1% vs. 4.5%; P < .01), individuals with lower household incomes (8.9% for <$20,000 vs. 6.0% for >$20,000; P < .01), and those with a history of a serious chronic condition (P = .05). After adjustment for these factors, along with prior smoking status and a history of radiation therapy, underweight survivors had an increased risk of all-cause mortality within 2 years of BMI report (OR, 2.85; P < .01), compared with ideal-weight survivors.
- CCSS investigators identified treatment-related risk factors for being underweight, including TBI (females) or abdominal irradiation (males), use of alkylating agents, and use of anthracyclines.[118]
Overweight/obesity
- To date, patients with cancer who have an increased incidence of being affected by overweight and obesity are primarily ALL [117,120,121,122,123,124] and CNS tumor [41,98] survivors who were treated with cranial radiation therapy.[118,125]
- The development of overweight/obesity after cranial radiation therapy is multifactorial and includes the following:[122,126,127]
- Growth hormone deficiency.
- Leptin sensitivity.
- Reduced levels of physical activity and energy expenditure.
Evidence (risk factors for overweight/obesity):
- In the nationwide Dutch Childhood Cancer Survivor Study (DCCSS-LATER) cohort of adult survivors of childhood cancer (n = 2,338), investigators found that having excess body weight (BMI >2.5 kg/m2) occurred in almost one-half of all long-term survivors. This incidence was not increased compared with the general population.[128]
- Overweight incidence was higher in women aged 50 years and older, and morbid obesity incidence was higher in men aged 50 years and older.
- Factors such as having excess body weight at cancer diagnosis, receiving cranial irradiation, and having growth hormone deficiency were all associated with long-term overweight status. Corticosteroids were not associated with overweight status.
- Dual-energy x-ray absorptiometry–based classification identified overweight in an additional 30% of survivors, particularly those treated with abdominal irradiation, TBI, anthracyclines, and platinum chemotherapy.
- CCSS investigators reported the following independent risk factors for obesity in childhood cancer survivors including treatment, lifestyle, and medication use:[129]
- Cancer diagnosed at ages 5 to 9 years (RR, 1.12; 95% CI, 1.01–1.24).
- Abnormal physical functioning (RR, 1.19; 95% CI, 1.06–1.33).
- Hypothalamic-pituitary radiation dose of 20 Gy to 30 Gy (RR, 1.17; 95% CI, 1.05–1.3; P = .01).
- Specific antidepressant use of paroxetine (RR, 1.29; 95% CI, 1.08–1.54).
- Survivors who adhered to the U.S. Centers for Disease Control and Prevention guidelines for vigorous physical activity (RR, 0.90; 95% CI, 0.82–0.97; P = .01) and who had a medium amount of anxiety (RR, 0.86; 95% CI, 0.75–0.99; P = .04) had a lower risk of obesity.[129]
Body composition alterations after childhood ALL
Evidence (risk factors for body composition alterations):
- Moderate-dose cranial radiation therapy (18–24 Gy) among ALL survivors is associated with obesity, particularly in females treated at a young age.[120,122,130]
- Female adult survivors of childhood ALL who were treated with cranial radiation therapy of 24 Gy before age 5 years are four times more likely to be affected by obesity than are women who have not been treated for a cancer.[120]
- Women treated with 18 Gy to 24 Gy cranial radiation therapy before age 10 years have a substantially greater rate of increase in their BMI through their young adult years than do women who were treated for ALL with only chemotherapy or women in the general population.[122]
- These women also have a significantly increased visceral adiposity and associated insulin resistance.[131,132]
- Body composition alterations appear to be attenuated in males.
- A study of long-term male survivors of ALL (mean age, 29 years) observed significantly higher body adiposity than in age-matched controls, despite normal weight and BMI.[133]
- Potential indicators of increased adiposity included high leptin and low sex hormone–binding globulin levels.[133]
- Serum testicular endocrine markers (testosterone, FSH, or inhibin B) did not correlate with body adiposity.[133]
- ALL therapy regimens are associated with increases in BMI shortly after completion of therapy, and possibly with a higher risk of obesity in the long term.[123,124,134,135,136]
- Several studies have reported that survivors of childhood ALL treated with chemotherapy alone also exhibit long-term changes in body composition, with relative increases in body fat [132,137,138,139] and visceral adiposity in comparison to lean mass.[131]
- These changes cannot be detected if BMI alone is used in the assessment of metabolic risk in this population.
- A genetic predisposition to excess adiposity may be enhanced when a child with ALL is treated with cranial irradiation. Genetic determinants of BMI identified in the general population were investigated in two large cohorts of childhood cancer survivors (n = 1,458) (CCSS and SJLIFE study).[140]
- Among ALL survivors who were treated with cranial radiation therapy in childhood, investigators identified statistical interactions of cranial radiation therapy treatment in survivors with germline genetic variants known to affect the baseline genetic risk of adiposity. This suggests that a genetic predisposition to excess adiposity may be enhanced when an individual is treated with cranial radiation therapy for childhood ALL.
Evidence (body composition changes in adult survivors of childhood ALL):
- A cohort study of 365 adult survivors of ALL (149 treated with cranial radiation therapy and 216 treated without cranial radiation therapy) compared body composition, energy balance, and fitness with age-, sex-, and race-matched peers.[141]
- Female survivors who were not exposed to cranial irradiation had comparable body composition values to that of peers.
- Waist circumference, waist-to-height ratio, total fat mass, and percent fat mass were higher among male survivors and cranial radiation–exposed female survivors than among comparison group members.
- Survivors of both sexes exposed to cranial radiation therapy had higher BMI and percent body fat than did survivors not exposed to cranial radiation therapy.
- Although survivors who did not receive cranial radiation therapy had energy balances similar to the matched peer group, they had significantly higher measures of impaired fitness (impaired flexibility, peripheral sensorimotor deficits, proximal muscle weakness, and poor exercise tolerance).
- In a CCSS study that was based on self-reported height and weight measurements, the following was observed:
- Swiss investigators evaluated self-reported weight in 1,936 adult survivors of childhood ALL, non-Hodgkin lymphoma, and Hodgkin lymphoma (median age, 24 years; median time from diagnosis, 17 years) and compared them with siblings and the general population.[142]
- The proportion of survivors who reported being overweight (26%) was comparable to that of siblings (24%) and the general Swiss population (25%).
- There was no evidence of a relationship between cumulative glucocorticoid dose and being overweight.
- There was also no evidence that the use of cranial radiation therapy modified the effect of the cumulative glucocorticoid dose on being overweight.
Variable outcomes across studies likely relate to the use of BMI as the metric for abnormal body composition, which does not adequately assess visceral adiposity that can contribute to metabolic risk in this population.[143]
Body composition alterations after treatment for CNS tumors
Among brain tumor survivors treated with higher doses of cranial radiation therapy, the highest risk of developing obesity has been observed in females treated at a younger age.[144]
Survivors of craniopharyngioma have a substantially increased risk of developing extreme obesity because of the tumor location and the hypothalamic damage resulting from surgical resection.[145,146,147,148]
A cohort of 661 childhood survivors of brain tumors (mean follow-up time, 7.3 years) was evaluated for weight gain associated with hypothalamic-pituitary dysfunction. This cohort excluded survivors who had craniopharyngiomas or pituitary tumors.[149]
- Among survivors between the ages of 4 and 20 years at follow-up, 20.3% were classified as overweight and 8.5% had obesity, compared with 10.5% and 2.7%, respectively, in the general Dutch population of comparable age.
- Hypothalamic-pituitary dysfunction was more prevalent in survivors who are overweight or have obesity than in survivors of normal weight.
- BMI SDS at diagnosis, diagnosis of low-grade glioma, and history of diabetes insipidus and central precocious puberty were associated with weight gain, being overweight, or having obesity.
Body composition alterations after HSCT
- Survivors of childhood cancer treated with TBI in preparation for an allogeneic HSCT have increased measures of body fatness (percent fat) while often having a normal BMI.[113,150,151,152]
- Longitudinal decline in BMI related to substantial decrease in lean mass has been observed among survivors of hematological malignancies treated with allogeneic HSCT.[153]
- This finding was largely attributable to TBI conditioning and severity of chronic GVHD.[153]
Body composition alterations after solid malignancies
- Survivors of abdominal and pelvic solid tumors treated with radiation therapy are at risk of alterations in body composition and metabolic health that can adversely affect functional performance.
- Among 431 survivors of childhood abdominal or pelvic tumors (median attained age, 29.9 years), higher cumulative doses of abdominal and pelvic radiation therapy were associated with lower lean muscle mass in both males and females.[154]
- Compared with survivors who have normal (high) lean mass and normal (low) fat mass, survivors with normal lean mass and high fat mass had a significantly higher risk of insulin resistance, low HDL cholesterol, reduced quadriceps strength, and reduced distance covered in a 6-minute walk.[154]
Body composition and frailty
Young adult survivors of childhood cancer have a higher-than-expected prevalence of frailty, a phenotype characterized by low muscle mass, self-reported exhaustion, low energy expenditure, slow walking speed, and weakness.[155]
- Individuals are considered prefrail if they have two of these five characteristics and frail if they have three or more of these characteristics.[155]
- The frailty phenotype increases in prevalence with aging, and has been associated with excess risk of mortality and onset of chronic conditions.[155]
- In CCSS participants, the overall prevalence of frailty among survivors (6.4%) was three times higher than that of sibling controls (2.2%).[156]
- The highest prevalence of frailty was reported in survivors of CNS tumors (9.5%) and bone tumors (8.1%).
- Cranial radiation, pelvic radiation (≥34 Gy), and lung surgery were independent risk factors for frailty in the CCSS cohort.
- In SJLIFE study participants (median age at study entry, 30 years), frailty prevalence increased from 6.2% to 13.6% during the 5 years of follow-up.[157]
- Risk factors for frailty at follow-up included treatment with chest radiation therapy of 20 Gy or higher (OR, 1.98), cardiac (OR, 1.58) and neurological (OR, 2.58) conditions, lack of strength training (OR, 1.74), sedentary lifestyle (OR, 1.75), and frailty at study entry (OR, 11.12).
- Prior history of frailty was the strongest risk factor for death during follow-up (OR, 3.52).
- In an SJLIFE study (follow-up interval, 5 years), young-adult survivors of childhood cancer who are considered prefrail and frail (n = 205) experienced significant declines in neurocognitive domains commonly associated with dementia and Alzheimer disease.[158]
- Survivors considered frail declined more on tests of short-term verbal recall and executive function than did survivors not considered frail.
- Survivors considered frail and prefrail experienced greater declines in focused attention than did survivors not considered frail.
- The prevalence of and risk factors for prefrailty, frailty, and sarcopenia were evaluated in a DCCSS-LATER cross-sectional study of adult survivors (mean age, 33.1 years at participation) of childhood cancer who were treated between 1963 and 2001.[159]
- The prefrailty rate was 20.3%, the frailty rate was 7.4%, and the sarcopenia rate was 4.4%.
- Significant risk factors for prefrailty included the following:
- Being underweight (OR, 3.38; 95% CI, 1.92–5.95).
- Having obesity (OR, 1.67; 95% CI, 1.14–2.43).
- Exposure to cranial irradiation (OR, 2.07; 95% CI, 1.47–2.93).
- Exposure to TBI (OR, 3.17; 95% CI, 1.77–5.70).
- Exposure to cisplatin dose of at least 600 mg/m2 (OR, 3.75; 95% CI, 1.82–7.74).
- Having a growth hormone deficiency (OR, 2.25; 95% CI, 1.23–4.09).
- Having hyperthyroidism (OR, 3.72; 95% CI, 1.63–8.47).
- Low bone mineral density (OR for Z score ≤−1 and >-2, 1.80; 95% CI, 1.31–2.47 and OR for Z score ≤-2, 3.37; 95% CI, 2.20–5.15).
- Having a folic acid deficiency (OR, 1.87; 95% CI, 1.31–2.68).
- Significant risk factors for sarcopenia included the following:
- Male sex (OR, 4.56; 95% CI, 2.26–9.17).
- Having a lower BMI (continuous, OR, 0.52; 95% CI, 0.45–0.60).
- Exposure to cranial irradiation (OR, 3.87; 95% CI, 1.80–8.31).
- Exposure to TBI (OR, 4.52; 95% CI, 1.67–12.20).
- Having hypogonadism (OR, 3.96; 95% CI, 1.40–11.18).
- Having a growth hormone deficiency (OR, 4.66; 95% CI, 1.44–15.15).
- Having a vitamin B12 deficiency (OR, 6.26).
- Survivors of childhood cancer may experience accelerated biological aging, resulting in premature frailty and death. Investigators used the SJLIFE cohort to evaluate a panel of the best-evidenced and most-studied of the newest aging biomarkers. They included seven measures of biological age acceleration in their analysis. Adult survivors of childhood cancer from the SJLIFE cohort were compared with two other control groups (community controls and the National Health and Nutrition Examination Survey controls). The goal was to determine whether survivors of childhood cancer (n = 4,117) were biologically older and aging more rapidly than controls who have not had childhood cancer.[160]
- Survivors of cancer aged 5% faster per year and measured, on average, 0.6 to 6.44 years biologically older than community controls.
- Survivors were 5 to 16 years biologically older than expected, compared with adults of their chronological age at the population level.
- Survivors who were treated with HSCT and vinca alkaloid chemotherapy showed the fastest trajectories of biological aging.
- Biologically older and faster-aging survivors consistently and robustly had a higher risk of frailty and died earlier than those with slower biological aging.
- Ongoing research aims to elucidate the pathophysiology of frailty and develop/test interventions to prevent or reverse this condition.
Table 13 summarizes body composition late effects and the related health screenings.
| Predisposing Therapy | Potential Late Effects | Health Screening |
|---|---|---|
| BMI = body mass index. | ||
| a Adapted from theChildren's Oncology Group Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers. | ||
| Cranial radiation therapy | Overweight/obesity | Height, weight, BMI, blood pressure test |
| Laboratory tests: Fasting glucose and lipids | ||
For endocrine and metabolic syndrome late effects information, including risk factors, evaluation, and health counseling, see the Children's Oncology Group Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers.
References:
- Brignardello E, Felicetti F, Castiglione A, et al.: Endocrine health conditions in adult survivors of childhood cancer: the need for specialized adult-focused follow-up clinics. Eur J Endocrinol 168 (3): 465-72, 2013.
- Mostoufi-Moab S, Seidel K, Leisenring WM, et al.: Endocrine Abnormalities in Aging Survivors of Childhood Cancer: A Report From the Childhood Cancer Survivor Study. J Clin Oncol 34 (27): 3240-7, 2016.
- Clement SC, Schouten-van Meeteren AY, Boot AM, et al.: Prevalence and Risk Factors of Early Endocrine Disorders in Childhood Brain Tumor Survivors: A Nationwide, Multicenter Study. J Clin Oncol 34 (36): 4362-4370, 2016.
- Chemaitilly W, Li Z, Huang S, et al.: Anterior hypopituitarism in adult survivors of childhood cancers treated with cranial radiotherapy: a report from the St Jude Lifetime Cohort study. J Clin Oncol 33 (5): 492-500, 2015.
- González Briceño LG, Kariyawasam D, Samara-Boustani D, et al.: High Prevalence of Early Endocrine Disorders After Childhood Brain Tumors in a Large Cohort. J Clin Endocrinol Metab 107 (5): e2156-e2166, 2022.
- Clement SC, van Rijn RR, van Eck-Smit BL, et al.: Long-term efficacy of current thyroid prophylaxis and future perspectives on thyroid protection during 131I-metaiodobenzylguanidine treatment in children with neuroblastoma. Eur J Nucl Med Mol Imaging 42 (5): 706-15, 2015.
- Clement SC, van Eck-Smit BL, van Trotsenburg AS, et al.: Long-term follow-up of the thyroid gland after treatment with 131I-Metaiodobenzylguanidine in children with neuroblastoma: importance of continuous surveillance. Pediatr Blood Cancer 60 (11): 1833-8, 2013.
- Bombardieri E, Giammarile F, Aktolun C, et al.: 131I/123I-metaiodobenzylguanidine (mIBG) scintigraphy: procedure guidelines for tumour imaging. Eur J Nucl Med Mol Imaging 37 (12): 2436-46, 2010.
- Sharp SE, Trout AT, Weiss BD, et al.: MIBG in Neuroblastoma Diagnostic Imaging and Therapy. Radiographics 36 (1): 258-78, 2016 Jan-Feb.
- Clement SC, Tytgat GAM, van Trotsenburg ASP, et al.: Thyroid function after diagnostic 123I-metaiodobenzylguanidine in children with neuroblastic tumors. Ann Nucl Med 36 (6): 579-585, 2022.
- Verloop H, Louwerens M, Schoones JW, et al.: Risk of hypothyroidism following hemithyroidectomy: systematic review and meta-analysis of prognostic studies. J Clin Endocrinol Metab 97 (7): 2243-55, 2012.
- Zatelli MC, Lamartina L, Meringolo D, et al.: Thyroid nodule recurrence following lobo-isthmectomy: incidence, patient's characteristics, and risk factors. J Endocrinol Invest 41 (12): 1469-1475, 2018.
- Chemaitilly W, Li Z, Brinkman TM, et al.: Primary hypothyroidism in childhood cancer survivors: Prevalence, risk factors, and long-term consequences. Cancer 128 (3): 606-614, 2022.
- Bölling T, Geisenheiser A, Pape H, et al.: Hypothyroidism after head-and-neck radiotherapy in children and adolescents: preliminary results of the "Registry for the Evaluation of Side Effects After Radiotherapy in Childhood and Adolescence" (RiSK). Int J Radiat Oncol Biol Phys 81 (5): e787-91, 2011.
- Inskip PD, Veiga LHS, Brenner AV, et al.: Hypothyroidism after Radiation Therapy for Childhood Cancer: A Report from the Childhood Cancer Survivor Study. Radiat Res 190 (2): 117-132, 2018.
- Sklar C, Whitton J, Mertens A, et al.: Abnormalities of the thyroid in survivors of Hodgkin's disease: data from the Childhood Cancer Survivor Study. J Clin Endocrinol Metab 85 (9): 3227-32, 2000.
- Vatner RE, Niemierko A, Misra M, et al.: Endocrine Deficiency As a Function of Radiation Dose to the Hypothalamus and Pituitary in Pediatric and Young Adult Patients With Brain Tumors. J Clin Oncol 36 (28): 2854-2862, 2018.
- Aldrich KD, Horne VE, Bielamowicz K, et al.: Comparison of hypothyroidism, growth hormone deficiency, and adrenal insufficiency following proton and photon radiotherapy in children with medulloblastoma. J Neurooncol 155 (1): 93-100, 2021.
- Milano MT, Vargo JA, Yorke ED, et al.: Primary Hypothyroidism in Childhood Cancer Survivors Treated With Radiation Therapy: A PENTEC Comprehensive Review. Int J Radiat Oncol Biol Phys 119 (2): 482-493, 2024.
- Wheeler G, Grassberger C, Samers J, et al.: Central Endocrine Complications Among Childhood Cancer Survivors Treated With Radiation Therapy: A PENTEC Comprehensive Review. Int J Radiat Oncol Biol Phys 119 (2): 457-466, 2024.
- Gleeson HK, Darzy K, Shalet SM: Late endocrine, metabolic and skeletal sequelae following treatment of childhood cancer. Best Pract Res Clin Endocrinol Metab 16 (2): 335-48, 2002.
- Inskip PD, Veiga LHS, Brenner AV, et al.: Hyperthyroidism After Radiation Therapy for Childhood Cancer: A Report from the Childhood Cancer Survivor Study. Int J Radiat Oncol Biol Phys 104 (2): 415-424, 2019.
- Clausen CT, Hasle H, Holmqvist AS, et al.: Hyperthyroidism as a late effect in childhood cancer survivors - an Adult Life after Childhood Cancer in Scandinavia (ALiCCS) study. Acta Oncol 58 (2): 227-231, 2019.
- Bhatti P, Veiga LH, Ronckers CM, et al.: Risk of second primary thyroid cancer after radiotherapy for a childhood cancer in a large cohort study: an update from the childhood cancer survivor study. Radiat Res 174 (6): 741-52, 2010.
- Haddy N, El-Fayech C, Guibout C, et al.: Thyroid adenomas after solid cancer in childhood. Int J Radiat Oncol Biol Phys 84 (2): e209-15, 2012.
- Ronckers CM, Sigurdson AJ, Stovall M, et al.: Thyroid cancer in childhood cancer survivors: a detailed evaluation of radiation dose response and its modifiers. Radiat Res 166 (4): 618-28, 2006.
- Sigurdson AJ, Ronckers CM, Mertens AC, et al.: Primary thyroid cancer after a first tumour in childhood (the Childhood Cancer Survivor Study): a nested case-control study. Lancet 365 (9476): 2014-23, 2005 Jun 11-17.
- van Santen HM, Tytgat GA, van de Wetering MD, et al.: Differentiated thyroid carcinoma after 131I-MIBG treatment for neuroblastoma during childhood: description of the first two cases. Thyroid 22 (6): 643-6, 2012.
- Veiga LH, Lubin JH, Anderson H, et al.: A pooled analysis of thyroid cancer incidence following radiotherapy for childhood cancer. Radiat Res 178 (4): 365-76, 2012.
- Kovalchik SA, Ronckers CM, Veiga LH, et al.: Absolute risk prediction of second primary thyroid cancer among 5-year survivors of childhood cancer. J Clin Oncol 31 (1): 119-27, 2013.
- Vivanco M, Dalle JH, Alberti C, et al.: Malignant and benign thyroid nodules after total body irradiation preceding hematopoietic cell transplantation during childhood. Eur J Endocrinol 167 (2): 225-33, 2012.
- Li Z, Franklin J, Zelcer S, et al.: Ultrasound surveillance for thyroid malignancies in survivors of childhood cancer following radiotherapy: a single institutional experience. Thyroid 24 (12): 1796-805, 2014.
- Brignardello E, Felicetti F, Castiglione A, et al.: Ultrasound surveillance for radiation-induced thyroid carcinoma in adult survivors of childhood cancer. Eur J Cancer 55: 74-80, 2016.
- Clement SC, Kremer LCM, Verburg FA, et al.: Balancing the benefits and harms of thyroid cancer surveillance in survivors of Childhood, adolescent and young adult cancer: Recommendations from the international Late Effects of Childhood Cancer Guideline Harmonization Group in collaboration with the PanCareSurFup Consortium. Cancer Treat Rev 63: 28-39, 2018.
- Baran JA, Halada S, Bauer AJ, et al.: Thyroid Ultrasound Screening in Childhood Cancer Survivors following Radiotherapy. Horm Res Paediatr 97 (3): 243-253, 2024.
- Metzger ML, Howard SC, Hudson MM, et al.: Natural history of thyroid nodules in survivors of pediatric Hodgkin lymphoma. Pediatr Blood Cancer 46 (3): 314-9, 2006.
- Francis GL, Waguespack SG, Bauer AJ, et al.: Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 25 (7): 716-59, 2015.
- Sanders JE, Hoffmeister PA, Woolfrey AE, et al.: Thyroid function following hematopoietic cell transplantation in children: 30 years' experience. Blood 113 (2): 306-8, 2009.
- Cattoni A, Molinari S, Gaiero A, et al.: Thyroid Disorders Following Hematopoietic Stem Cell Transplantation in Childhood: Impact of Conditioning Regimen on Thyroid Dysfunction, Volume Changes, and Occurrence of Nodules. Transplant Cell Ther 28 (8): 506.e1-506.e12, 2022.
- van Iersel L, Mulder RL, Denzer C, et al.: Hypothalamic-Pituitary and Other Endocrine Surveillance Among Childhood Cancer Survivors. Endocr Rev 43 (5): 794-823, 2022.
- Gurney JG, Kadan-Lottick NS, Packer RJ, et al.: Endocrine and cardiovascular late effects among adult survivors of childhood brain tumors: Childhood Cancer Survivor Study. Cancer 97 (3): 663-73, 2003.
- Hudson MM, Ness KK, Gurney JG, et al.: Clinical ascertainment of health outcomes among adults treated for childhood cancer. JAMA 309 (22): 2371-81, 2013.
- Sklar CA, Antal Z, Chemaitilly W, et al.: Hypothalamic-Pituitary and Growth Disorders in Survivors of Childhood Cancer: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 103 (8): 2761-2784, 2018.
- Ramelli GP, von der Weid N, Stanga Z, et al.: Suprasellar germinomas in childhood and adolescence: diagnostic pitfalls. J Pediatr Endocrinol Metab 11 (6): 693-7, 1998 Nov-Dec.
- Vinchon M, Baroncini M, Leblond P, et al.: Morbidity and tumor-related mortality among adult survivors of pediatric brain tumors: a review. Childs Nerv Syst 27 (5): 697-704, 2011.
- Fahrner B, Prosch H, Minkov M, et al.: Long-term outcome of hypothalamic pituitary tumors in Langerhans cell histiocytosis. Pediatr Blood Cancer 58 (4): 606-10, 2012.
- Lawson SA, Horne VE, Golekoh MC, et al.: Hypothalamic-pituitary function following childhood brain tumors: Analysis of prospective annual endocrine screening. Pediatr Blood Cancer 66 (5): e27631, 2019.
- Lebbink CA, Ringers TP, Schouten-van Meeteren AYN, et al.: Prevalence and risk factors of hypothalamic-pituitary dysfunction in infant and toddler childhood brain tumor survivors. Eur J Endocrinol 185 (4): 597-606, 2021.
- Fraser O, Crowne E, Tacey M, et al.: Correlating measured radiotherapy dose with patterns of endocrinopathy: The importance of minimizing pituitary dose. Pediatr Blood Cancer 69 (11): e29847, 2022.
- van Iersel L, Li Z, Srivastava DK, et al.: Hypothalamic-Pituitary Disorders in Childhood Cancer Survivors: Prevalence, Risk Factors and Long-Term Health Outcomes. J Clin Endocrinol Metab 104 (12): 6101-6115, 2019.
- Darzy KH, Shalet SM: Hypopituitarism following radiotherapy. Pituitary 12 (1): 40-50, 2009.
- Viana MB, Vilela MI: Height deficit during and many years after treatment for acute lymphoblastic leukemia in children: a review. Pediatr Blood Cancer 50 (2 Suppl): 509-16; discussion 517, 2008.
- Merchant TE, Goloubeva O, Pritchard DL, et al.: Radiation dose-volume effects on growth hormone secretion. Int J Radiat Oncol Biol Phys 52 (5): 1264-70, 2002.
- Merchant TE, Rose SR, Bosley C, et al.: Growth hormone secretion after conformal radiation therapy in pediatric patients with localized brain tumors. J Clin Oncol 29 (36): 4776-80, 2011.
- Merchant TE, Wu S, Onar-Thomas A, et al.: Endocrinopathy After Treatment for Medulloblastoma: Results From the SJMB03 Trial of Risk-Adapted Radiation Therapy. Int J Radiat Oncol Biol Phys 116 (3): 560-568, 2023.
- van Iersel L, van Santen HM, Potter B, et al.: Clinical impact of hypothalamic-pituitary disorders after conformal radiation therapy for pediatric low-grade glioma or ependymoma. Pediatr Blood Cancer 67 (12): e28723, 2020.
- Sklar C, Mertens A, Walter A, et al.: Final height after treatment for childhood acute lymphoblastic leukemia: comparison of no cranial irradiation with 1800 and 2400 centigrays of cranial irradiation. J Pediatr 123 (1): 59-64, 1993.
- Chow EJ, Friedman DL, Yasui Y, et al.: Decreased adult height in survivors of childhood acute lymphoblastic leukemia: a report from the Childhood Cancer Survivor Study. J Pediatr 150 (4): 370-5, 375.e1, 2007.
- Vandecruys E, Dhooge C, Craen M, et al.: Longitudinal linear growth and final height is impaired in childhood acute lymphoblastic leukemia survivors after treatment without cranial irradiation. J Pediatr 163 (1): 268-73, 2013.
- Browne EK, Zhou Y, Chemaitilly W, et al.: Changes in body mass index, height, and weight in children during and after therapy for acute lymphoblastic leukemia. Cancer 124 (21): 4248-4259, 2018.
- Demoor-Goldschmidt C, Allodji RS, Journy N, et al.: Risk Factors for Small Adult Height in Childhood Cancer Survivors. J Clin Oncol 38 (16): 1785-1796, 2020.
- Mizumoto M, Oshiro Y, Pan H, et al.: Height after photon craniospinal irradiation in pediatric patients treated for central nervous system embryonal tumors. Pediatr Blood Cancer 67 (10): e28617, 2020.
- Ogilvy-Stuart AL, Clark DJ, Wallace WH, et al.: Endocrine deficit after fractionated total body irradiation. Arch Dis Child 67 (9): 1107-10, 1992.
- Willi SM, Cooke K, Goldwein J, et al.: Growth in children after bone marrow transplantation for advanced neuroblastoma compared with growth after transplantation for leukemia or aplastic anemia. J Pediatr 120 (5): 726-32, 1992.
- Wingard JR, Plotnick LP, Freemer CS, et al.: Growth in children after bone marrow transplantation: busulfan plus cyclophosphamide versus cyclophosphamide plus total body irradiation. Blood 79 (4): 1068-73, 1992.
- Huma Z, Boulad F, Black P, et al.: Growth in children after bone marrow transplantation for acute leukemia. Blood 86 (2): 819-24, 1995.
- Bernard F, Bordigoni P, Simeoni MC, et al.: Height growth during adolescence and final height after haematopoietic SCT for childhood acute leukaemia: the impact of a conditioning regimen with BU or TBI. Bone Marrow Transplant 43 (8): 637-42, 2009.
- Chemaitilly W, Sklar CA: Endocrine complications of hematopoietic stem cell transplantation. Endocrinol Metab Clin North Am 36 (4): 983-98; ix, 2007.
- Socié G, Salooja N, Cohen A, et al.: Nonmalignant late effects after allogeneic stem cell transplantation. Blood 101 (9): 3373-85, 2003.
- Cohen A, Rovelli A, Bakker B, et al.: Final height of patients who underwent bone marrow transplantation for hematological disorders during childhood: a study by the Working Party for Late Effects-EBMT. Blood 93 (12): 4109-15, 1999.
- Brennan BM, Shalet SM: Endocrine late effects after bone marrow transplant. Br J Haematol 118 (1): 58-66, 2002.
- Sfeir JG, Kittah NEN, Tamhane SU, et al.: Diagnosis of GH Deficiency as a Late Effect of Radiotherapy in Survivors of Childhood Cancers. J Clin Endocrinol Metab 103 (8): 2785-2793, 2018.
- Raman S, Grimberg A, Waguespack SG, et al.: Risk of Neoplasia in Pediatric Patients Receiving Growth Hormone Therapy--A Report From the Pediatric Endocrine Society Drug and Therapeutics Committee. J Clin Endocrinol Metab 100 (6): 2192-203, 2015.
- Chemaitilly W, Robison LL: Safety of growth hormone treatment in patients previously treated for cancer. Endocrinol Metab Clin North Am 41 (4): 785-92, 2012.
- Sklar CA, Mertens AC, Mitby P, et al.: Risk of disease recurrence and second neoplasms in survivors of childhood cancer treated with growth hormone: a report from the Childhood Cancer Survivor Study. J Clin Endocrinol Metab 87 (7): 3136-41, 2002.
- Ergun-Longmire B, Mertens AC, Mitby P, et al.: Growth hormone treatment and risk of second neoplasms in the childhood cancer survivor. J Clin Endocrinol Metab 91 (9): 3494-8, 2006.
- Patterson BC, Chen Y, Sklar CA, et al.: Growth hormone exposure as a risk factor for the development of subsequent neoplasms of the central nervous system: a report from the childhood cancer survivor study. J Clin Endocrinol Metab 99 (6): 2030-7, 2014.
- Bogarin R, Steinbok P: Growth hormone treatment and risk of recurrence or progression of brain tumors in children: a review. Childs Nerv Syst 25 (3): 273-9, 2009.
- Tamhane S, Sfeir JG, Kittah NEN, et al.: GH Therapy in Childhood Cancer Survivors: A Systematic Review and Meta-Analysis. J Clin Endocrinol Metab 103 (8): 2794-2801, 2018.
- Thomas-Teinturier C, Oliver-Petit I, Pacquement H, et al.: Influence of growth hormone therapy on the occurrence of a second neoplasm in survivors of childhood cancer. Eur J Endocrinol 183 (4): 471-480, 2020.
- Boguszewski MCS, Boguszewski CL, Chemaitilly W, et al.: Safety of growth hormone replacement in survivors of cancer and intracranial and pituitary tumours: a consensus statement. Eur J Endocrinol 186 (6): P35-P52, 2022.
- Chemaitilly W, Merchant TE, Li Z, et al.: Central precocious puberty following the diagnosis and treatment of paediatric cancer and central nervous system tumours: presentation and long-term outcomes. Clin Endocrinol (Oxf) 84 (3): 361-71, 2016.
- Armstrong GT, Whitton JA, Gajjar A, et al.: Abnormal timing of menarche in survivors of central nervous system tumors: A report from the Childhood Cancer Survivor Study. Cancer 115 (11): 2562-70, 2009.
- Didcock E, Davies HA, Didi M, et al.: Pubertal growth in young adult survivors of childhood leukemia. J Clin Oncol 13 (10): 2503-7, 1995.
- Shalet SM, Crowne EC, Didi MA, et al.: Irradiation-induced growth failure. Baillieres Clin Endocrinol Metab 6 (3): 513-26, 1992.
- Gan HW, Phipps K, Aquilina K, et al.: Neuroendocrine Morbidity After Pediatric Optic Gliomas: A Longitudinal Analysis of 166 Children Over 30 Years. J Clin Endocrinol Metab 100 (10): 3787-99, 2015.
- Chemaitilly W, Sklar CA: Endocrine complications in long-term survivors of childhood cancers. Endocr Relat Cancer 17 (3): R141-59, 2010.
- Greulich WW, Pyle SI: Radiographic Atlas of Skeletal Development of Hand and Wrist. 2nd ed. Stanford University Press, 1959.
- Gleeson HK, Stoeter R, Ogilvy-Stuart AL, et al.: Improvements in final height over 25 years in growth hormone (GH)-deficient childhood survivors of brain tumors receiving GH replacement. J Clin Endocrinol Metab 88 (8): 3682-9, 2003.
- Laughton SJ, Merchant TE, Sklar CA, et al.: Endocrine outcomes for children with embryonal brain tumors after risk-adapted craniospinal and conformal primary-site irradiation and high-dose chemotherapy with stem-cell rescue on the SJMB-96 trial. J Clin Oncol 26 (7): 1112-8, 2008.
- Bielamowicz K, Okcu MF, Sonabend R, et al.: Hypothyroidism after craniospinal irradiation with proton or photon therapy in patients with medulloblastoma. Pediatr Hematol Oncol 35 (4): 257-267, 2018.
- van Iersel L, Xu J, Potter BS, et al.: Clinical Importance of Free Thyroxine Concentration Decline After Radiotherapy for Pediatric and Adolescent Brain Tumors. J Clin Endocrinol Metab 104 (11): 4998-5007, 2019.
- Kazlauskaite R, Evans AT, Villabona CV, et al.: Corticotropin tests for hypothalamic-pituitary- adrenal insufficiency: a metaanalysis. J Clin Endocrinol Metab 93 (11): 4245-53, 2008.
- Rose SR, Danish RK, Kearney NS, et al.: ACTH deficiency in childhood cancer survivors. Pediatr Blood Cancer 45 (6): 808-13, 2005.
- Clement SC, Peeters RP, Ronckers CM, et al.: Intermediate and long-term adverse effects of radioiodine therapy for differentiated thyroid carcinoma--a systematic review. Cancer Treat Rev 41 (10): 925-34, 2015.
- Follin C, Erfurth EM: Long-Term Effect of Cranial Radiotherapy on Pituitary-Hypothalamus Area in Childhood Acute Lymphoblastic Leukemia Survivors. Curr Treat Options Oncol 17 (9): 50, 2016.
- Rensen N, Gemke RJ, van Dalen EC, et al.: Hypothalamic-pituitary-adrenal (HPA) axis suppression after treatment with glucocorticoid therapy for childhood acute lymphoblastic leukaemia. Cochrane Database Syst Rev 11 (11): CD008727, 2017.
- Constine LS, Woolf PD, Cann D, et al.: Hypothalamic-pituitary dysfunction after radiation for brain tumors. N Engl J Med 328 (2): 87-94, 1993.
- Constine LS, Rubin P, Woolf PD, et al.: Hyperprolactinemia and hypothyroidism following cytotoxic therapy for central nervous system malignancies. J Clin Oncol 5 (11): 1841-51, 1987.
- Melmed S, Casanueva FF, Hoffman AR, et al.: Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 96 (2): 273-88, 2011.
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III): Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 106 (25): 3143-421, 2002.
- Bolier M, de Winter DTC, Pluimakers VG, et al.: Prevalence and determinants of metabolic syndrome in 2338 childhood cancer survivors: A Dutch Childhood Cancer Survivor LATER 2 study. Cancer 131 (1): e35681, 2025.
- Saultier P, Auquier P, Bertrand Y, et al.: Metabolic syndrome in long-term survivors of childhood acute leukemia treated without hematopoietic stem cell transplantation: an L.E.A. study. Haematologica 101 (12): 1603-1610, 2016.
- Nottage KA, Ness KK, Li C, et al.: Metabolic syndrome and cardiovascular risk among long-term survivors of acute lymphoblastic leukaemia - From the St. Jude Lifetime Cohort. Br J Haematol 165 (3): 364-74, 2014.
- Oudin C, Berbis J, Bertrand Y, et al.: Prevalence and characteristics of metabolic syndrome in adults from the French childhood leukemia survivors' cohort: a comparison with controls from the French population. Haematologica 103 (4): 645-654, 2018.
- van Waas M, Neggers SJ, Raat H, et al.: Abdominal radiotherapy: a major determinant of metabolic syndrome in nephroblastoma and neuroblastoma survivors. PLoS One 7 (12): e52237, 2012.
- Smith WA, Li C, Nottage KA, et al.: Lifestyle and metabolic syndrome in adult survivors of childhood cancer: a report from the St. Jude Lifetime Cohort Study. Cancer 120 (17): 2742-50, 2014.
- Jones LW, Liu Q, Armstrong GT, et al.: Exercise and risk of major cardiovascular events in adult survivors of childhood hodgkin lymphoma: a report from the childhood cancer survivor study. J Clin Oncol 32 (32): 3643-50, 2014.
- Scott JM, Li N, Liu Q, et al.: Association of Exercise With Mortality in Adult Survivors of Childhood Cancer. JAMA Oncol 4 (10): 1352-1358, 2018.
- Baker KS, Ness KK, Steinberger J, et al.: Diabetes, hypertension, and cardiovascular events in survivors of hematopoietic cell transplantation: a report from the bone marrow transplantation survivor study. Blood 109 (4): 1765-72, 2007.
- van Waas M, Neggers SJ, Uitterlinden AG, et al.: Treatment factors rather than genetic variation determine metabolic syndrome in childhood cancer survivors. Eur J Cancer 49 (3): 668-75, 2013.
- de Vathaire F, El-Fayech C, Ben Ayed FF, et al.: Radiation dose to the pancreas and risk of diabetes mellitus in childhood cancer survivors: a retrospective cohort study. Lancet Oncol 13 (10): 1002-10, 2012.
- Armenian SH, Chemaitilly W, Chen M, et al.: National Institutes of Health Hematopoietic Cell Transplantation Late Effects Initiative: The Cardiovascular Disease and Associated Risk Factors Working Group Report. Biol Blood Marrow Transplant 23 (2): 201-210, 2017.
- Lega IC, Pole JD, Austin PC, et al.: Diabetes Risk in Childhood Cancer Survivors: A Population-Based Study. Can J Diabetes 42 (5): 533-539, 2018.
- Baker KS, Chow EJ, Goodman PJ, et al.: Impact of treatment exposures on cardiovascular risk and insulin resistance in childhood cancer survivors. Cancer Epidemiol Biomarkers Prev 22 (11): 1954-63, 2013.
- Meacham LR, Chow EJ, Ness KK, et al.: Cardiovascular risk factors in adult survivors of pediatric cancer--a report from the childhood cancer survivor study. Cancer Epidemiol Biomarkers Prev 19 (1): 170-81, 2010.
- van Santen HM, Geskus RB, Raemaekers S, et al.: Changes in body mass index in long-term childhood cancer survivors. Cancer 121 (23): 4197-204, 2015.
- Meacham LR, Gurney JG, Mertens AC, et al.: Body mass index in long-term adult survivors of childhood cancer: a report of the Childhood Cancer Survivor Study. Cancer 103 (8): 1730-9, 2005.
- Tonorezos ES, Chou JF, Moskowitz CS, et al.: Risk of increased mortality in underweight survivors: A brief report from the Childhood Cancer Survivor Study. Pediatr Blood Cancer 71 (8): e31080, 2024.
- Oeffinger KC, Mertens AC, Sklar CA, et al.: Obesity in adult survivors of childhood acute lymphoblastic leukemia: a report from the Childhood Cancer Survivor Study. J Clin Oncol 21 (7): 1359-65, 2003.
- Sklar CA, Mertens AC, Walter A, et al.: Changes in body mass index and prevalence of overweight in survivors of childhood acute lymphoblastic leukemia: role of cranial irradiation. Med Pediatr Oncol 35 (2): 91-5, 2000.
- Garmey EG, Liu Q, Sklar CA, et al.: Longitudinal changes in obesity and body mass index among adult survivors of childhood acute lymphoblastic leukemia: a report from the Childhood Cancer Survivor Study. J Clin Oncol 26 (28): 4639-45, 2008.
- Chow EJ, Pihoker C, Hunt K, et al.: Obesity and hypertension among children after treatment for acute lymphoblastic leukemia. Cancer 110 (10): 2313-20, 2007.
- Withycombe JS, Post-White JE, Meza JL, et al.: Weight patterns in children with higher risk ALL: A report from the Children's Oncology Group (COG) for CCG 1961. Pediatr Blood Cancer 53 (7): 1249-54, 2009.
- Nathan PC, Jovcevska V, Ness KK, et al.: The prevalence of overweight and obesity in pediatric survivors of cancer. J Pediatr 149 (4): 518-25, 2006.
- Oeffinger KC: Are survivors of acute lymphoblastic leukemia (ALL) at increased risk of cardiovascular disease? Pediatr Blood Cancer 50 (2 Suppl): 462-7; discussion 468, 2008.
- Brennan BM, Rahim A, Blum WF, et al.: Hyperleptinaemia in young adults following cranial irradiation in childhood: growth hormone deficiency or leptin insensitivity? Clin Endocrinol (Oxf) 50 (2): 163-9, 1999.
- Pluimakers VG, van Atteveld JE, de Winter DTC, et al.: Prevalence, risk factors, and optimal way to determine overweight, obesity, and morbid obesity in the first Dutch cohort of 2338 long-term survivors of childhood cancer: a DCCSS-LATER study. Eur J Endocrinol 189 (5): 495-507, 2023.
- Green DM, Cox CL, Zhu L, et al.: Risk factors for obesity in adult survivors of childhood cancer: a report from the Childhood Cancer Survivor Study. J Clin Oncol 30 (3): 246-55, 2012.
- Veringa SJ, van Dulmen-den Broeder E, Kaspers GJ, et al.: Blood pressure and body composition in long-term survivors of childhood acute lymphoblastic leukemia. Pediatr Blood Cancer 58 (2): 278-82, 2012.
- Janiszewski PM, Oeffinger KC, Church TS, et al.: Abdominal obesity, liver fat, and muscle composition in survivors of childhood acute lymphoblastic leukemia. J Clin Endocrinol Metab 92 (10): 3816-21, 2007.
- Oeffinger KC, Adams-Huet B, Victor RG, et al.: Insulin resistance and risk factors for cardiovascular disease in young adult survivors of childhood acute lymphoblastic leukemia. J Clin Oncol 27 (22): 3698-704, 2009.
- Jahnukainen K, Heikkinen R, Henriksson M, et al.: Increased Body Adiposity and Serum Leptin Concentrations in Very Long-Term Adult Male Survivors of Childhood Acute Lymphoblastic Leukemia. Horm Res Paediatr 84 (2): 108-15, 2015.
- Dalton VK, Rue M, Silverman LB, et al.: Height and weight in children treated for acute lymphoblastic leukemia: relationship to CNS treatment. J Clin Oncol 21 (15): 2953-60, 2003.
- Kohler JA, Moon RJ, Wright S, et al.: Increased adiposity and altered adipocyte function in female survivors of childhood acute lymphoblastic leukaemia treated without cranial radiation. Horm Res Paediatr 75 (6): 433-40, 2011.
- Zhang FF, Rodday AM, Kelly MJ, et al.: Predictors of being overweight or obese in survivors of pediatric acute lymphoblastic leukemia (ALL). Pediatr Blood Cancer 61 (7): 1263-9, 2014.
- Warner JT, Evans WD, Webb DK, et al.: Body composition of long-term survivors of acute lymphoblastic leukaemia. Med Pediatr Oncol 38 (3): 165-72, 2002.
- Miller TL, Lipsitz SR, Lopez-Mitnik G, et al.: Characteristics and determinants of adiposity in pediatric cancer survivors. Cancer Epidemiol Biomarkers Prev 19 (8): 2013-22, 2010.
- Jarfelt M, Lannering B, Bosaeus I, et al.: Body composition in young adult survivors of childhood acute lymphoblastic leukaemia. Eur J Endocrinol 153 (1): 81-9, 2005.
- Richard MA, Brown AL, Belmont JW, et al.: Genetic variation in the body mass index of adult survivors of childhood acute lymphoblastic leukemia: A report from the Childhood Cancer Survivor Study and the St. Jude Lifetime Cohort. Cancer 127 (2): 310-318, 2021.
- Ness KK, DeLany JP, Kaste SC, et al.: Energy balance and fitness in adult survivors of childhood acute lymphoblastic leukemia. Blood 125 (22): 3411-9, 2015.
- Belle FN, Kasteler R, Schindera C, et al.: No evidence of overweight in long-term survivors of childhood cancer after glucocorticoid treatment. Cancer 124 (17): 3576-3585, 2018.
- Lindemulder SJ, Stork LC, Bostrom B, et al.: Survivors of standard risk acute lymphoblastic leukemia do not have increased risk for overweight and obesity compared to non-cancer peers: a report from the Children's Oncology Group. Pediatr Blood Cancer 62 (6): 1035-41, 2015.
- Gurney JG, Ness KK, Stovall M, et al.: Final height and body mass index among adult survivors of childhood brain cancer: childhood cancer survivor study. J Clin Endocrinol Metab 88 (10): 4731-9, 2003.
- Sahakitrungruang T, Klomchan T, Supornsilchai V, et al.: Obesity, metabolic syndrome, and insulin dynamics in children after craniopharyngioma surgery. Eur J Pediatr 170 (6): 763-9, 2011.
- Müller HL: Childhood craniopharyngioma: current controversies on management in diagnostics, treatment and follow-up. Expert Rev Neurother 10 (4): 515-24, 2010.
- Simoneau-Roy J, O'Gorman C, Pencharz P, et al.: Insulin sensitivity and secretion in children and adolescents with hypothalamic obesity following treatment for craniopharyngioma. Clin Endocrinol (Oxf) 72 (3): 364-70, 2010.
- Tosta-Hernandez PDC, Siviero-Miachon AA, da Silva NS, et al.: Childhood Craniopharyngioma: A 22-Year Challenging Follow-Up in a Single Center. Horm Metab Res 50 (9): 675-682, 2018.
- van Schaik J, van Roessel IMAA, Schouten-van Meeteren NAYN, et al.: High Prevalence of Weight Gain in Childhood Brain Tumor Survivors and Its Association With Hypothalamic-Pituitary Dysfunction. J Clin Oncol 39 (11): 1264-1273, 2021.
- Neville KA, Cohn RJ, Steinbeck KS, et al.: Hyperinsulinemia, impaired glucose tolerance, and diabetes mellitus in survivors of childhood cancer: prevalence and risk factors. J Clin Endocrinol Metab 91 (11): 4401-7, 2006.
- Nysom K, Holm K, Michaelsen KF, et al.: Degree of fatness after allogeneic BMT for childhood leukaemia or lymphoma. Bone Marrow Transplant 27 (8): 817-20, 2001.
- Ketterl TG, Chow EJ, Leisenring WM, et al.: Adipokines, Inflammation, and Adiposity in Hematopoietic Cell Transplantation Survivors. Biol Blood Marrow Transplant 24 (3): 622-626, 2018.
- Inaba H, Yang J, Kaste SC, et al.: Longitudinal changes in body mass and composition in survivors of childhood hematologic malignancies after allogeneic hematopoietic stem-cell transplantation. J Clin Oncol 30 (32): 3991-7, 2012.
- Wilson CL, Liu W, Chemaitilly W, et al.: Body Composition, Metabolic Health, and Functional Impairment among Adults Treated for Abdominal and Pelvic Tumors during Childhood. Cancer Epidemiol Biomarkers Prev 29 (9): 1750-1758, 2020.
- Ness KK, Krull KR, Jones KE, et al.: Physiologic frailty as a sign of accelerated aging among adult survivors of childhood cancer: a report from the St Jude Lifetime cohort study. J Clin Oncol 31 (36): 4496-503, 2013.
- Hayek S, Gibson TM, Leisenring WM, et al.: Prevalence and Predictors of Frailty in Childhood Cancer Survivors and Siblings: A Report From the Childhood Cancer Survivor Study. J Clin Oncol 38 (3): 232-247, 2020.
- Delaney A, Howell CR, Krull KR, et al.: Progression of Frailty in Survivors of Childhood Cancer: A St. Jude Lifetime Cohort Report. J Natl Cancer Inst 113 (10): 1415-1421, 2021.
- Williams AM, Krull KR, Howell CR, et al.: Physiologic Frailty and Neurocognitive Decline Among Young-Adult Childhood Cancer Survivors: A Prospective Study From the St Jude Lifetime Cohort. J Clin Oncol 39 (31): 3485-3495, 2021.
- van Atteveld JE, de Winter DTC, Pluimakers VG, et al.: Frailty and sarcopenia within the earliest national Dutch childhood cancer survivor cohort (DCCSS-LATER): a cross-sectional study. Lancet Healthy Longev 4 (4): e155-e165, 2023.
- Guida JL, Hyun G, Belsky DW, et al.: Associations of seven measures of biological age acceleration with frailty and all-cause mortality among adult survivors of childhood cancer in the St. Jude Lifetime Cohort. Nat Cancer 5 (5): 731-741, 2024.

