How It Is Done
Catheter ablation
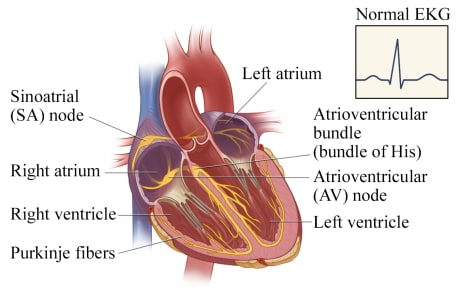
In a normal heart, the sinoatrial (SA) node triggers the electrical impulse, causing the upper chambers (atria) to contract. The signal travels through the atrioventricular (AV) node to the atrioventricular bundle, which divides into the Purkinje fibers that carry the signal and cause the lower chambers (ventricles) to contract. The electrocardiogram (EKG, ECG) tracing shows this normal electrical activity.
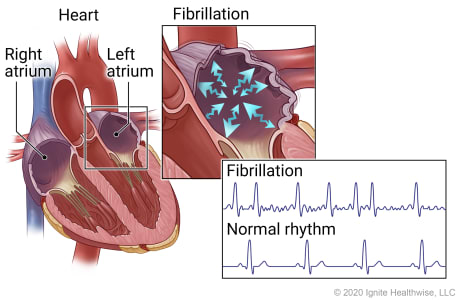
In atrial fibrillation, erratic electrical impulses can cause the upper chambers of the heart (atria) to fibrillate, or quiver, resulting in an irregular and frequently rapid heart rate. The irregular, sawtooth pattern in the electrocardiogram (EKG, ECG) tracing shows these erratic impulses.
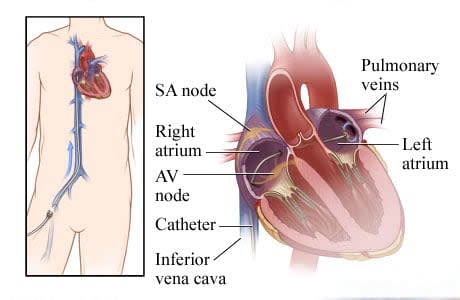
For this nonsurgical procedure called catheter ablation, thin tubes called catheters are inserted into a vein, typically in the groin or neck, and threaded through the vein into the heart. A small puncture in the tissue that divides the right and left chambers (septum) allows the catheter to pass into the left atrium.
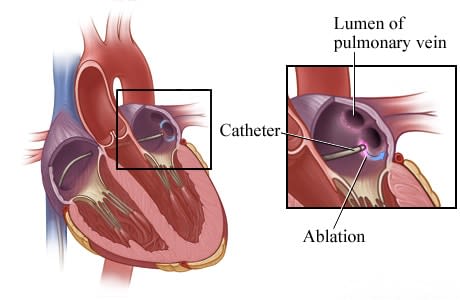
An electrode at the tip of a catheter sends out energy that destroys (ablates) the tissue that is causing atrial fibrillation. The main types of ablation are:
Thermal ablation. This is the most common type of heart ablation. It uses either heat (radiofrequency) or extreme cold (cryoablation) to destroy the small areas of heart tissue causing the abnormal rhythm.
Pulsed field ablation (PFA). PFA uses short, high-voltage electrical pulses to target and destroy only the heart cells causing the abnormal rhythm. Since it only targets the problem areas, PFA may lower the risk of damage to nearby areas like the esophagus, nerves, or blood vessels.
In this image, the energy is destroying tissue at the base of the pulmonary vein. (The pulmonary veins bring blood back from the lungs to the heart.)
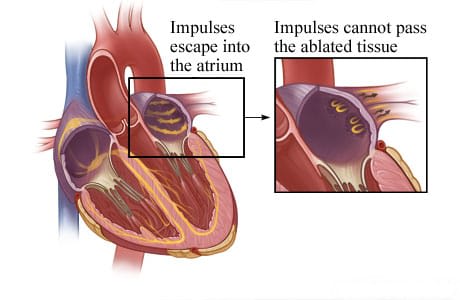
Catheter ablation creates scar tissue that prevents impulses from leaving the pulmonary veins or eliminates the impulses altogether.
AV node ablation
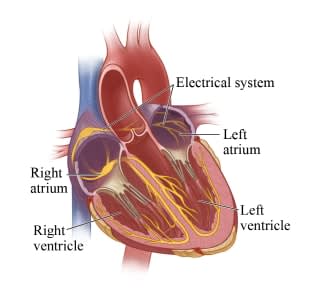
In a normal heart, electrical impulses pace the rhythm at which the heart contracts and relaxes. The sinoatrial (SA) node triggers the electrical impulse, causing the upper chambers (atria) to contract. The signal travels through the atrioventricular (AV) node to the atrioventricular bundle, which divides into the Purkinje fibers that carry the signal and cause the lower chambers (ventricles) to contract. The electrocardiogram (EKG, ECG) shows this normal electrical activity.
In atrial fibrillation, erratic electrical impulses in the upper chambers of the heart (atria) cause those chambers to fibrillate, or quiver. This results in an irregular and frequently rapid heart rate. The irregular, sawtooth pattern in the electrocardiogram (EKG, ECG) shows these erratic impulses.
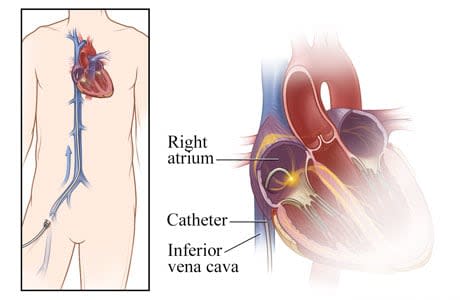
For this nonsurgical procedure, catheters are inserted into a vein, typically in the groin or neck, and threaded through the vena cava vein into the right atrium of the heart.
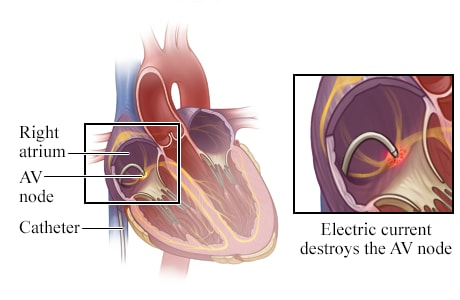
An electrode at the tip of the catheter sends out energy—such as radio waves, very cold temperatures, or laser light—that destroys (ablates) the atrioventricular (AV) node or other heart tissue that is responsible for the erratic impulses.
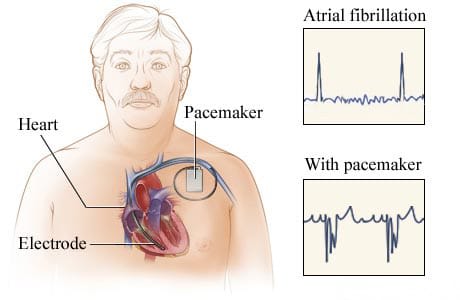
When the AV node is ablated, a permanent pacemaker is implanted that paces the ventricle. The pulse generator and battery part of the pacemaker are implanted under the skin of the chest. The electrocardiograms (EKG, ECG) show the heart's electrical activity during atrial fibrillation and when a heart has a pacemaker.
What To Expect
You may stay in the hospital overnight. You may have swelling, bruising, or a small lump around the site where the catheters went into your body. You can do light activities at home. Don't do anything strenuous until your doctor says it is okay. This may be for several days.
Many people think that having ablation means they'll be able to stop taking an anticoagulant every day to prevent stroke. But that is only true if your risk of stroke is low. Studies haven't proved that ablation for atrial fibrillation lowers your risk of stroke. So you'll still need to take an anticoagulant if your risk of stroke remains high. Your doctor can tell you about your stroke risk.
After an ablation, you might take an antiarrhythmic medicine for a few months to help keep your heart in a normal rhythm.
Your doctor might ask you to take your pulse at home to see if it's irregular. You might also use an ambulatory EKG monitor (such as a Holter monitor) at home to check your heart rhythm.
You might feel symptoms, such as palpitations, after the ablation procedure. These symptoms might happen while your heart is healing. Sometimes the symptoms may feel different to you after the ablation compared to before the ablation. During your follow-up visits, tell your doctor if you have symptoms. If they don't go away after a few months, you may choose to have a second ablation procedure.
Watch

Current as of: October 2, 2025
Author: Ignite Healthwise, LLC Staff
Clinical Review Board
All Ignite Healthwise, LLC education is reviewed by a team that includes physicians, nurses, advanced practitioners, registered dieticians, and other healthcare professionals.







